
False Lumen Coil Embolization for Persistent Pain Following TEVAR for Type B Dissection
Julia Glaser, MD, Seth Concors, MD, Wilson Szeto, MD, Matthew Williams, MD, Venkat Kalapatapu, MD.
University of Pennsylvania, Philadelphia, PA, USA.
OBJECTIVES: To describe the use of false lumen coil embolization for persistent back pain following TEVAR.
METHODS:: Retrospective chart review was used to describe two cases of false lumen coil embolization. Coil embolizations were performed to treat a persistent false lumen and back pain after TEVAR performed for type B dissection.
RESULTS: The first patient was a 71-year-old female who presented with an acute type B dissection. She failed conservative management due to persistent back pain, and underwent an uncomplicated left carotid-subclavian bypass followed by a TEVAR and left subclavian coil embolization. She was discharged, and subsequently re-presented 3 weeks later with persistent back pain and radiologic evidence of false lumen filling. Medical management was unsuccessful, so the false lumen of her dissection was coil embolized. This produced thrombosis of the thoracic false lumen and resolution of her back pain. CTA performed 6 months after the initial TEVAR and 4 months after the coil embolization shows favorable remodeling. The second patient was a 54 year-old-female who presented with an acute type B dissection with a diameter of 6.2 cm. Her TEVAR was complicated by a retrograde type A dissection, and she underwent a total arch replacement. She recovered well, and was discharged, but presented in follow-up with persistent filling of the false lumen and back pain. Proximal extension of the TEVAR along with left carotid subclavian bypass and left subclavian embolization failed to resolve her back pain, so she underwent false lumen coil embolization. This produced thrombosis of the false lumen, and resolution of the back pain. Follow-up imaging, now approximately two years after embolization, shows continued false lumen thrombosis.
CONCLUSIONS: Coil embolization of a persistent false lumen after TEVAR for type B dissection can produce false lumen thrombosis. This is a useful adjunct to promote favorable aortic remodeling and can help resolve symptoms.FIGURE LEGEND: A) Intra-operative picture showing coils being placed into the false lumen of patient 2 and B) CTA obtained at the 1 month follow up visit showing false lumen thrombosis. 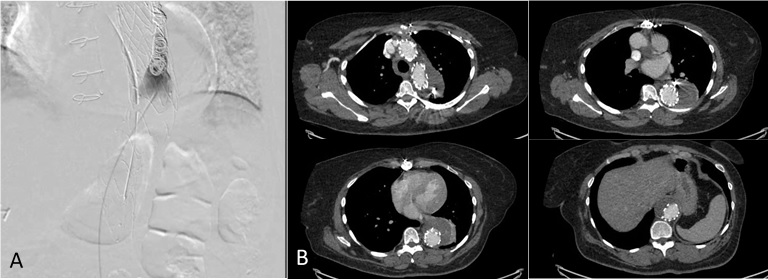
Back to 2018 ePosters



