
Economic Burden and Clinical Impact of Opioid Dependence in Patients Undergoing Lower Extremity Bypass Surgery: Quantifying the Cost of a New Epidemic
Matthew Aizpuru, BA, Kevin X. Farley, BS, Lindsay K. Gallo, BA, Eric R. Wagner, MD, William D. Jordan, Jr., MD, Jaime Benarroch-Gampel, MD, Robert S. Crawford, MD.
Emory University, Atlanta, GA, USA.
Objective:
Surgeons’ contributions to the opioid epidemic have received significant attention in the media. Little data exists, however, on the impact of prior or coexistent opioid use on vascular surgery outcomes. This study aims to quantify the economic impact of pre-existing opioid dependency in patients undergoing lower extremity bypass surgery.
Methods:
Data were collected from 1,132,317 patient admissions for lower extremity bypass in the National Inpatient Sample from years 2002-2015. Patients with a concomitant diagnosis of opioid abuse or dependency were identified using ICD-9 codes. Matched cohorts of patients with and without opioid dependence were created using coarsened exact matching to control for patient demographics. Linear regression was used to control for hospital-level factors and identify differential outcomes for patients with opioid dependency.
Results:
3,189 (0.3%) patients undergoing lower extremity bypass were found to have a concomitant opioid use disorder. The incidence of opioid dependency rose over time [0.13% (2002); 0.63% (2015), p<.001, fig. 1]. Before matching, opioid dependent patients were younger (53.9 ± 12.3 yrs vs. 66.7 ± 12.1 yrs, p<.001), more likely to be male (65.2% vs. 61.9%, p<.001), non-white (37.9% vs 24.1%, p<.001), pay with Medicaid (29.6% vs 7.4%, p<.001), and fall in the lowest income quartile based on zip code (39.6% vs 27.5%, p<.001). After matching, there was no difference in in-hospital mortality (1.7% vs. 2.1%, p=0.5), MI (2.1% vs 2.4%, p=0.7), PE (0.8% vs 0.4%, p=.08) or amputation (2.4% vs. 1.8%, p=.16). Opioid dependent patients were more likely to have surgical site infections (12.0% vs 5.9%, p<.001), septicemia (5.0% vs 3.3%, p=.03) and acute renal failure (13.0% vs. 8.2%, p<.001). Linear regression of matched cohorts revealed opioid dependent patients had an increased length of stay (12.5 days vs. 9.1 days, p<.001) and increased mean inflation-adjusted cost of $10,608 ($40,127 vs. $29,519 p<.001).
Conclusions:
Patients with opioid use disorder undergoing lower extremity bypass surgery have staggering increases in length of hospital stay and costs. Furthermore, the rise in the incidence of opioid dependency highlights the importance of early pre-operative recognition of this disorder in patients undergoing vascular surgery, and opens the opportunity for early intervention. 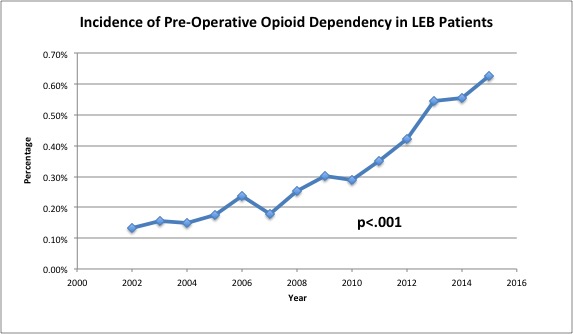
Back to 2019 Abstracts