
Lessons learned from the removal of thrombosed inferior vena cava filters
Limael Rodriguez, David J. Dexter, MD, Animesh Rathore, MD, Tomas Mesar, MD, Fanny Alie-Cusson, MD, Gordon K. Stokes, MD, Jean M. Panneton, MD.
Eastern Virginia Medical School, Norfolk, VA, USA.
OBJECTIVES: Thrombosis of inferior vena cava filters (IVCF) is a well described complication that can occur in up to 20% despite adherence to anticoagulation. In this study, we review our experience with symptomatic IVCF thrombosis and report outcomes with IVCF removal.
METHODS: A retrospective chart review of all patients with a diagnosis of symptomatic thrombosed IVCF ± IFDVT (iliofemoral deep vein thrombosis) that underwent IVCF removal since September 2014 was performed. The primary endpoints were technical success, recurrent DVT, PE, and mortality.
RESULTS: Overall, 9 patients (mean age, 60 years, range 35-77, M/F 7/9) underwent IVC filter removal. Patients presented with IVC thrombosis with either concomitant bilateral IFDVT in 5/9 (56%) or single segment IFDVT 4/9 (44%). Of these, 2/9 (22%) were acute symptom onset (≤14 days evolution), 5/9 (56%) were subacute (15-45 days), and two patients were chronic (>45 days). The mean time since placement was 802 days (range: 66-5268; median: 347). Overall, 5/9 (56%) filters were retrievable and 3/9 (22%) were permanent. Multiple advanced intraoperative techniques (i.e. balloon, double snare, and/or loop techniques) to assist in removal were used with a mean operative time of 130 min (range: 60-230). Technical success for endovascular approach was 8/9 (89%), and one patient required a planned open removal after multiple failed endovascular attempts. Concomitant CDT+PMT was used in 6/9 (67%) patients, one patient received CDT alone, and two patients required angioplasty for chronic IVC occlusion. There were no 30 day postoperative major adverse events or mortality. There were no readmissions related to IVC occlusion at one year follow up. Two patients (22%) were treated within one year for recurrent IFDVT without IVC involvement.
CONCLUSIONS: In patients with symptomatic IVCF thrombosis, explantation is technically challenging but feasible with good technical success. The procedure usually requires advanced thrombectomy and removal techniques, but can be performed with low perioperative complications. When combined with postoperative oral anticoagulation therapy, we experienced a low incidence of recurrent thrombosis.
Figure 1. Thrombosed IVC filter after successful retrieval on first attempt. Although the filter is disfigured, no fractures in the filter or residual pieces (on completion radiograph) were noted. 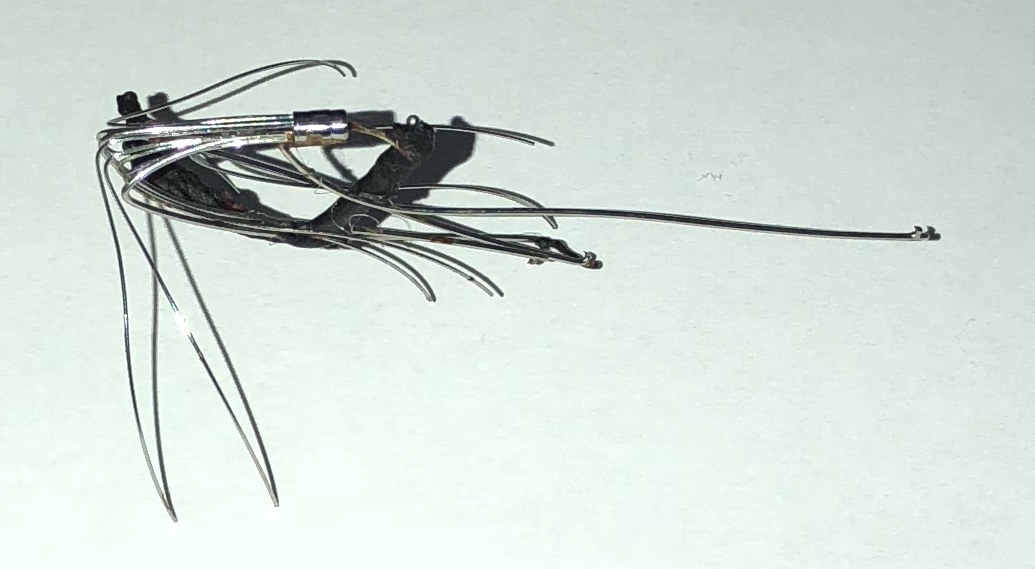
Back to 2019 Abstracts