
Retrograde Open Mesenteric Stenting as a Treatment of Acute Iatrogenic Mesenteric Occlusion in Endovascular Repair of Abdominal Aortic Aneurysm
Heepeel Chang, MD, Neal C. Hadro, MD, Marc A. Norris, MD, Marvin E. Morris, MD.
Baystate Medical Center, University of Massachusetts Medical School, Springfield, MA, USA.
OBJECTIVES: Retrograde open mesenteric stenting (ROMS) has evolved as a useful technical adjunct for revascularization in mesenteric ischemia. The hybrid mesenteric revascularization with exploratory laparotomy to directly expose the mesenteric artery and establish distal mesenteric artery access to deploy a stent across the atherosclerotic lesion has gained popularity. To add to that body of literature, we describe the successful use of ROMS in the setting of iatrogenic mesenteric occlusion during EVAR.
METHODS: The clinical data and outcomes of patients who underwent ROMS and EVAR from 2011 to 2018 were retrospectively reviewed at a tertiary care medical center. All patient underwent an exploratory laparotomy followed by retrograde balloon angioplasty and stenting using an iCAST balloon-expandable covered stent (Atrium Medical Corp., Merrimack, NH). End points were technical success, patency rate, freedom from symptom recurrence or reintervention and mortality at 6-month.
RESULTS: There were two male patients with a mean age of 83.5 years. Indications for ROMS were as follows: 1. In the 76-year old with celiac stenosis, prior superior mesenteric artery (SMA) stent was occluded during EVAR with Ovation® endograft (Endologix Inc, Irvine, CA); 2. In the 91-year old, SMA occlusion occurred while realigning of prior EVAR with AFX® device (Endologix Inc, Irvine, CA) using aorto-uni-iliac device (Cook Medical, Bloomington, IN) for a contained AAA rupture secondary to type IIIa endoleak. Both patients underwent successful SMA stenting with a mean treatment length of 38 mm. Bowel resection was not needed in these patients. Technical success was achieved in all patients. At 6-month, patency rate and freedom from recurrence and re-intervention were 100%. The 91-year old died of overwhelming sepsis from a femoral-to-femoral graft infection at 7-month postoperatively.
CONCLUSIONS: ROMS can be utilized as a useful technical adjunct for iatrogenic mesenteric occlusion in EVAR. This report expands the literature to utility of ROMS in complex EVARS with inadvertent SMA coverage.
FIGURE: A. Intraoperative angiogram showing occlusion of SMA with patent celiac artery (arrow). B. Angiogram revealing open retrograde SMA stent deployment (arrow). C. Completion angiogram illustrating patent SMA stent (arrow). D. Postoperative sagittal slice of CTA at 6-month demonstrating patent SMA stent (arrow). 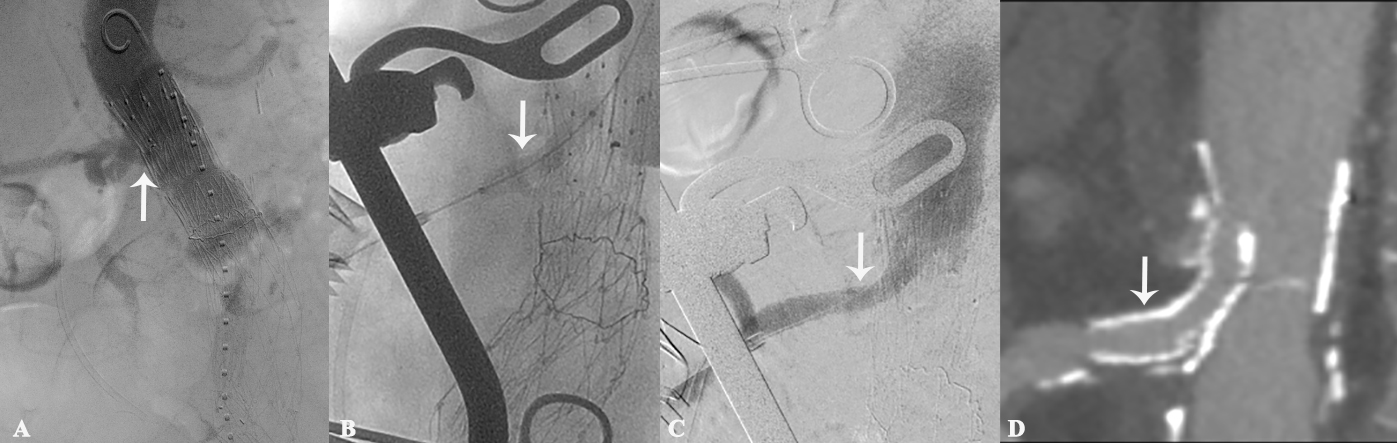
Back to 2019 ePosters