
Fenestrated Endovascular Aneurysm Repair with Concomitant Horseshoe Kidney
Danielle Peters, MS1, Melissa Obmann, DO1, Boyoung Song, MD1, Shivprasad Nikam, MD1, Evan Ryer, MD2, David Mariner, MD1.
1Geisinger Wyoming Valley Medical Center, Wilkes-Barre, PA, USA, 2Geisinger Medical Center, Danville, PA, USA.
Objective:
Horseshoe kidney (HSK) is a rare anomaly posing surgical challenges in the setting of abdominal aortic aneurysm (AAA) repair. Technical challenges associated with open surgical approaches and limited endovascular options due to variable arterial blood supply, lend controversy to which surgical method is most suitable for repair of AAA with concomitant HSK (AAA-HSK). We present a case in which a custom fenestrated endograft was used to accommodate a large mid-aortic renal artery supplying the isthmus of a HSK.
Methods:
A 60-year-old male with normal renal function and known HSK presented for elective repair of a 5.3 cm AAA. Preoperative computed tomography angiography (CTA) showed Eisendrath type 3 HSK with a large renal artery arising from mid-aorta, supplying the isthmus, and two renal arteries for both sides of the HSK. After confirming anatomic suitability, a custom fenestrated stent graft was designed to accommodate the large mid-aortic renal artery to avoid sacrifice of any parenchymal circulation.
Results:
Following bilateral percutaneous femoral access, a 20 French sheath was passed up the right femoral artery. The sheath was doubly accessed using 6 French sheath. The proximal main body device (Cook Medical Zenith® Fenestrated Graft, Bloomington Indiana) was advanced from left femoral access into the peri-visceral aorta. The graft was positioned to align the fenestration and the main body was partially deployed. The mid-aortic renal artery was selected and long sheath placed. Main body deployment was completed and fixation achieved with a balloon. Next, a 6 mm balloon expandable covered stent was deployed in the mid-aortic renal artery and "flared" open. The distal main body and iliac limbs were inserted and deployed in standard fashion. Completion imaging showed perfusion to the entire HSK with no obvious endoleak. The patient recovered well with normal renal function and was discharged. CTA performed at one month showed stable repair with preserved flow to the HSK and small type 2 endoleak.
Conclusions:
If the prerequisites of anatomic suitability and normal renal function are fulfilled, fenestrated endovascular aneurysm repair (FEVAR) is an excellent option in the presence of AAA-HSK. 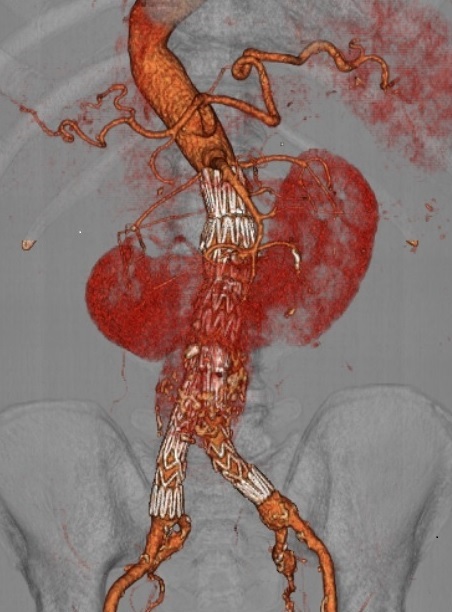
Back to 2019 ePosters