
Aneurysm of the Anterior Tibial Artery
Neha Sheng, M.D., Rebecca A. Deal, M.D., Erin C. Farlow, M.D., Richard Keen, M.D..
John. H. Stroger Hospital of Cook County, Chicago, IL, USA.
DEMOGRAPHICS A 40 year-old man was diagnosed with infective endocarditis and an anterior tibial artery aneurysm.
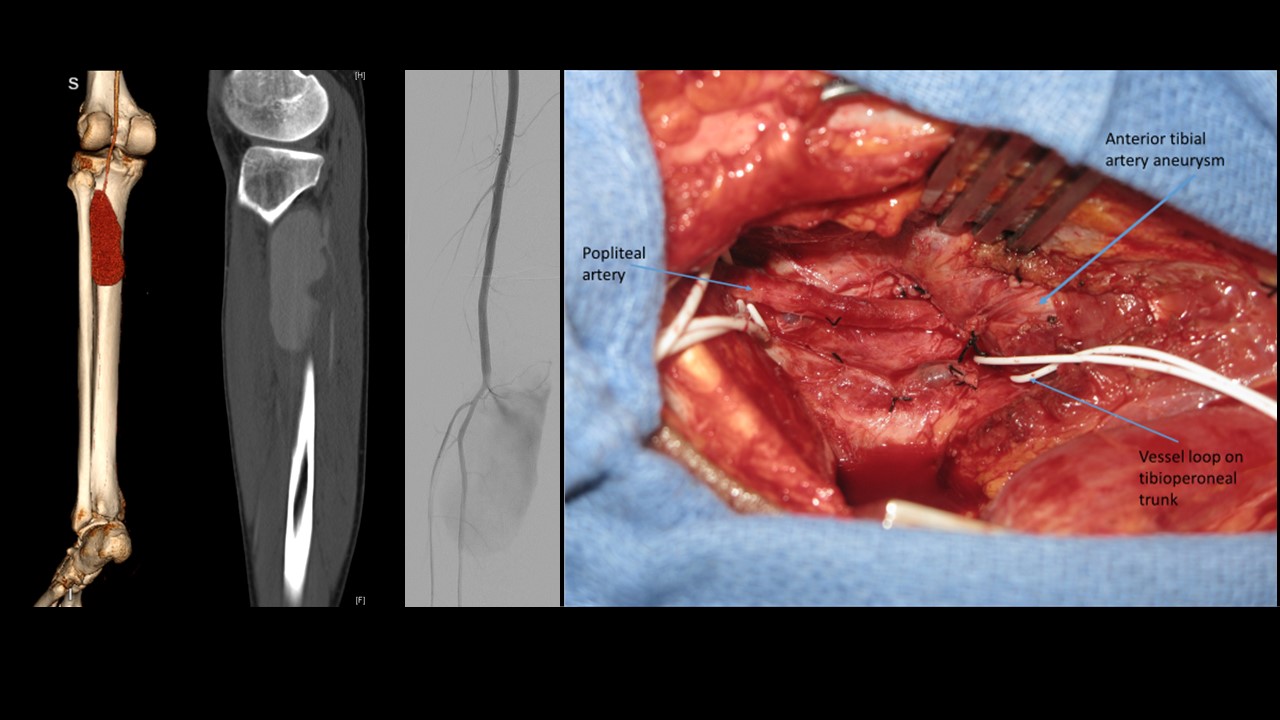
HISTORY A 40-year-old man presented for treatment of progressive shortness of breath and left lower extremity swelling and pain for 4 weeks. The patient had a history of asthma and smoking cigarettes. He had no history of trauma, claudication, recent travel, intravenous drug use, congestive heart failure, or an immunocompromised state. On physical exam, he was noted to have signs of congestive heart failure and left lower extremity edema with tenderness to palpation on left posterior leg. His posterior tibial and dorsalis pedis pulses were slightly diminished on the left compared to the right. Initial laboratory studies demonstrated leukocytosis. His initial blood cultures grew Cardiobacterium hominis. A venous duplex ultrasound showed no deep venous thrombus. Computed tomography angiogram (CTA) of the left lower extremity revealed a 10.3x3.2 cm aneurysm arising from the proximal left anterior tibial artery. A conventional angiogram confirmed the diagnosis. Transesophageal echocardiogram (TEE) revealed severe mitral valve regurgitation, severe aortic valve regurgitation and aortic valve vegetations.
PLAN The patient underwent successful aortic valve and mitral valve replacement. The following day, he underwent anterior tibial artery aneurysm resection. Using a medial approach, the infrageniculate popliteal artery was controlled. The anterior tibial artery and tibioperoneal trunk were also controlled proximally. The size of the aneurysm and its location in the anterior compartment precluded distal control, medially. The distal anterior tibial artery was controlled through a lateral leg incision, and the aneurysm was excised. Given healthy appearance of the vessel wall at the origin of the anterior tibial artery, a primary repair was done. The popliteal artery and tibioperoneal trunk were reapproximated with interrupted 6-0 prolene sutures, in a transverse fashion. Both the dorsalis pedis and the posterior tibial artery pulses remained palpable. His postoperative sensorimotor examination was normal. Culture of the anterior tibial artery aneurysm wall had no bacterial growth.
DISCUSSION: Few cases of anterior tibial artery aneurysms have been reported in the past. The combined medial and lateral approach is an effective way to surgically manage proximal anterior tibial artery aneurysms.
Back to 2019 ePosters