
Left Internal Mammary Artery Access for Embolization of the Left sSubclavian Artery in a Patient with Type II Endoleak after TEVAR for Ruptured Right-sided Aortic Arch Aneurysm : a Novel Approach
Fanny Alie-Cusson, MD, Sami M. Abou-Assi, Limael E. Rodriguez, MD, Djurabek Babadjanov, MD, Animesh Rathore, MD, Jean M. Panneton, MD.
Eastern Virginia Medical School, Norfolk, VA, USA.
Demographics
Type II endoleaks after thoracic endovascular aortic repair (TEVAR) can arise in up to 20% of patients. Locating the source of the endoleak and treating the culprit back-bleeding branch can be challenging. We present a case of percutaneous left internal mammary artery (LIMA) access for treatment of type II endoleak after a complex hybrid repair in a patient with ruptured right-sided aortic arch aneurysm (RSAAA) and aberrant left subclavian artery (LSA) associated with Kommerell’s diverticulum (KD).
History
A 65-year-old previously healthy woman presented to our emergency department with a one-week history of back pain after a fall. A CT angiogram (CTA) revealed a ruptured type B intramural hematoma (IMH) associated with RSAAA and a large KD at the aberrant LSCA origin. The patient underwent a total aortic arch replacement with elephant trunk (ET) and TEVAR under deep hypothermic circulatory arrest. Intra-operatively, the LSA was ligated distal to the origin of the left vertebral artery (LVA) with bypass to the axillary artery. On post-operative day 7, she developed hemorrhagic anemia due to a brisk type II endoleak into KD via retrograde flow from the LVA, confirmed on CTA.
Plan
Given the patient's prior proximal LSA ligation, options were limited to address this endoleak. Open options were a more proximal LSA ligation via a supraclavicular exposure or a redo median sternotomy. Endovascular access for coil embolization of the proximal LSA was also limited given the ligation of the LSA distal to LVA. Percutaneous access of the LIMA from left 4th intercostal space and coil embolization of the proximal LSA and KD was ultimately performed. This successfully treated the type II endoleak. 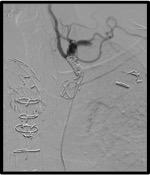 Patient was discharged on POD #26. On one-year follow-up, the patient remains asymptomatic and CTA revealed no evidence of endoleak with complete thoracic remodeling.
Patient was discharged on POD #26. On one-year follow-up, the patient remains asymptomatic and CTA revealed no evidence of endoleak with complete thoracic remodeling.
Discussion
RSAAA with aberrant LSA and associated Kommerell’s diverticulum is a rare occurrence. Our patient presenting with rupture was successfully managed with total arch debranching with FET and TEVAR. This case illustrates the novel use of the LIMA as an alternative access for LSA embolization in patients with type II endoleak and limited access options.
Back to 2019 ePosters