
Ligation of Left sided IVC during Open Repair of Ruptured Juxtarenal Abdominal Aortic Aneurysm.
Yoko M. Young Sang, Chiranjiv S. Virk, Robert K. White, Vyas R. Rao, Miles Sugar, Muzammil Aziz.
Lousiana State University Shreveport, Shreveport, LA, USA.
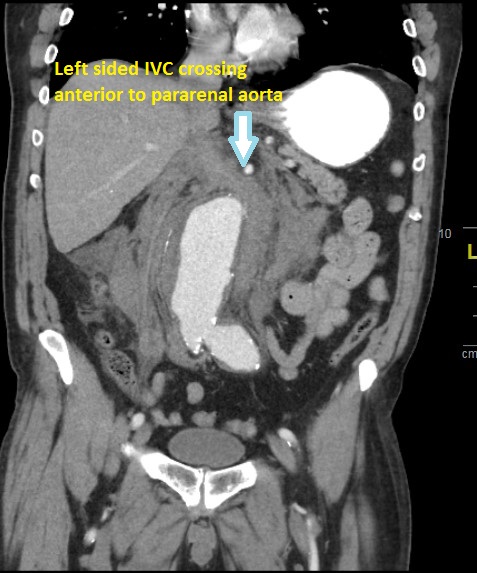
DEMOGRAPHICS 67 years old Caucasian Male. HISTORY Patient presented with sudden onset severe back pain at outside hospital. Past medical history was significant for Coronary Artery Disease, Hypertension, and Chronic Kidney Disease stage 3. Past surgical history was significant for Coronary Artery Bypass Grafting and Appendectomy. A Computed Tomography (CT) scan with IV contrast showed a contained rupture of juxtarenal Abdominal Aortic Aneurysm (AAA) (6.7cm) with an associated 4cm left common iliac artery aneurysm. Patient had stable vital signs with normal mentation. PLAN Open repair was elected as most suitable treatment option given juxtarenal nature of pathology. Midline laparotomy approach was performed with cross clamping of suprarenal aorta. Exposure to suprarenal aorta was complicated by a large left sided Inferior Vena Cava (IVC) crossing over to join right renal vein. It was divided after ligating with a transverse 30 mm linear vascular stapler. Aortobiliac repair performed excluding both abdominal and left common iliac artery aneurysms. Coagulopathy was encountered towards end of the procedure. Post op course complicated by re-exploration on post op day (POD1) for bleeding and biological mesh repair for fascial dehiscence on POD 7. Continued bilateral lower extremities swelling and presence of massive iliofemoral DVT on venous duplex ultrasound prompted venogram of bilateral lower extremity on POD 14, confirming the diagnosis of thrombosed single left sided IVC. CT venogram showed open left renal vein draining though tributaries in addition to thrombosed left sided IVC. Conservative management with anticoagulation and SCDs resulted in complete resolution of symptoms of bilateral lower extremity swelling. Follow up at 8 months revealed no signs or symptoms of venous insufficiency.
DISCUSSION Identification of left inferior vena cava anomalies with venous reconstruction performed at the index operation during open repair of intact or rupture abdominal aortic aneurysm have been described in literature. To our knowledge this is first described case report of ligation of left sided IVC during an open repair of ruptured juxtarenal AAA managed successfully with conservative measures. In the absence of clinical evidence of phlegmasia this approach should be considered when dealing with an unstable and tenuous patient.
Back to 2019 ePosters