
The Profunda Femoris Artery: A Rare Source of Type II Endoleak
Kelly A. Poirier, DO, Michael Amendola, MD, John Pfeifer, MD.
VA Medical Center/VCU Health System, Richmond, VA, USA.
Demographics:
Patient is an 80-year-old African American male with past medical history including a 3.6 x 4.5 cm abdominal aortic aneurysm and right 2.6 x 3.1 cm and left 3.7 cm iliac artery aneurysms. He underwent staged bilateral hypogastric artery embolization in 2009. An endograft was then placed with post-operative CTA showing a Type II endoleak in the left hypogastric with a stable aneurysm diameter of 4.0 over several years.
History:
The patient was followed yearly with CT scan and duplex examinations. He was found to have a new Type 1b endoleak in 2016 with a size increase of the left iliac aneurysm from 3.7 cm to 4.4 cm. The patient underwent diagnostic angiogram which showed only a Type II Endoleak originating from two branches of the profunda femoris artery (Figure 1). Due to the complexity of these branches, they were ligated in an open approach. Repeat intra-operative angiogram confirmed ligation. Post-operatively, his left iliac arterial aneurysm remained stable at 4.3 cm. The patient presented two years later with evidence of a recurrent endoleak. An angiogram with left common femoral arterial access demonstrates a recurrent Type II from a branch of the profunda femoris artery.
PLAN
The patient is a complicated surgical candidate with multiple co-morbidities. He will undergo pre-operative cardiac and pulmonary clearance and will likely require further open ligation of these perforating branches to prevent increased dilation of his aneurysm.
DISCUSSION
Endoleaks are a well-described complication associated with endovascular aneurysm repair (EVAR), with Type II Endoleaks being the most common sub-type. This subgroup may be further divided into those with single vessel involvement or multiple vessels involvement, and persistent Type II Endoleak predictors include patients with increased collateralization. Review of the literature confirms common femoral artery can be a source of these endoleaks but to date the profunda femoris artery has yet to be reported let alone in a recurrent fashion. 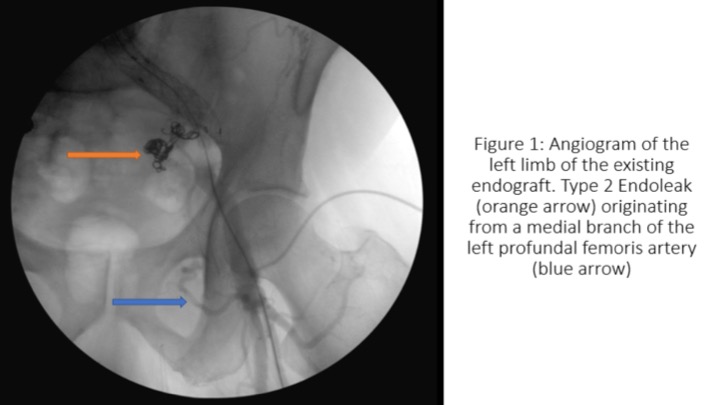
Back to 2019 ePosters