
Recurrent Polymicrobial Bloodstream Infections as Harbingers of a Duodenal-Inferior Vena Cava Fistula
Gregory Koval, MD, Benjamin Grams, MD, Richard Hankins, MD, Jasmine Marcelin, MD, Luciano Vargas, MD, Nitin Garg, MD.
UNMC, Omaha, NE, USA.
OBJECTIVES: Duodenal-caval fistula (DCF) is rare and associated with a high mortality. This discussion highlights DCF as an uncommon complication of IVC stenting and describes the presentation and repair.METHODS: We report a case of an 82-year-old female patient with multiple medical comorbidities who previously underwent distal IVC to common iliac vein stenting for post thrombotic syndrome. The patient presented with recurrent polymicrobial bloodstream infections and no obvious source of infection. CT scans demonstrated a small amount of gas within the lumen of the IVC stent that was initially thought to be from IV access. No other signs of infection were present in the surrounding tissue. Enteroscopy failed to show any abnormalities. DCF was suspected given recurrent bloodstream infections in the context of suspicious intraluminal air. The patient was taken to the OR for exploratory laparotomy and suspected DCF repair. The duodenum was found to be adherent to the IVC with a communication between them (Figure 1). The duodenum was repaired primarily in two layers. The segment of the stent was occluded and partially removed and the IVC wall was excised. IVC reconstruction was avoided due to the patient’s clinical status. With no saphenous veins available, a fascia lata patch was used to repair the IVC and covered with an omental pedicle flap. She was discharged on post-operative day 10. At one month, the patient was doing well clinically with no further bloodstream infections. A CT showed no concerns for DCF recurrence. RESULTS: Our case has certain unique elements. We thought that the reason for infection was the enteric communication and not primary stent infection and with the source removed and antibiotics, bare metal stents would allow infection control. A fascia lata patch was utilized to repair the fistula with successful outcome. We have utilized this as reinforcement for aortic repair in an infected field. The character of tissue, assumed resistance to infection, and relative ease of harvest made this an ideal choice for this case. CONCLUSIONS: This is a unique case that highlights a previously unreported complication of IVC stenting, the challenges in diagnosis and complex treatment decisions. 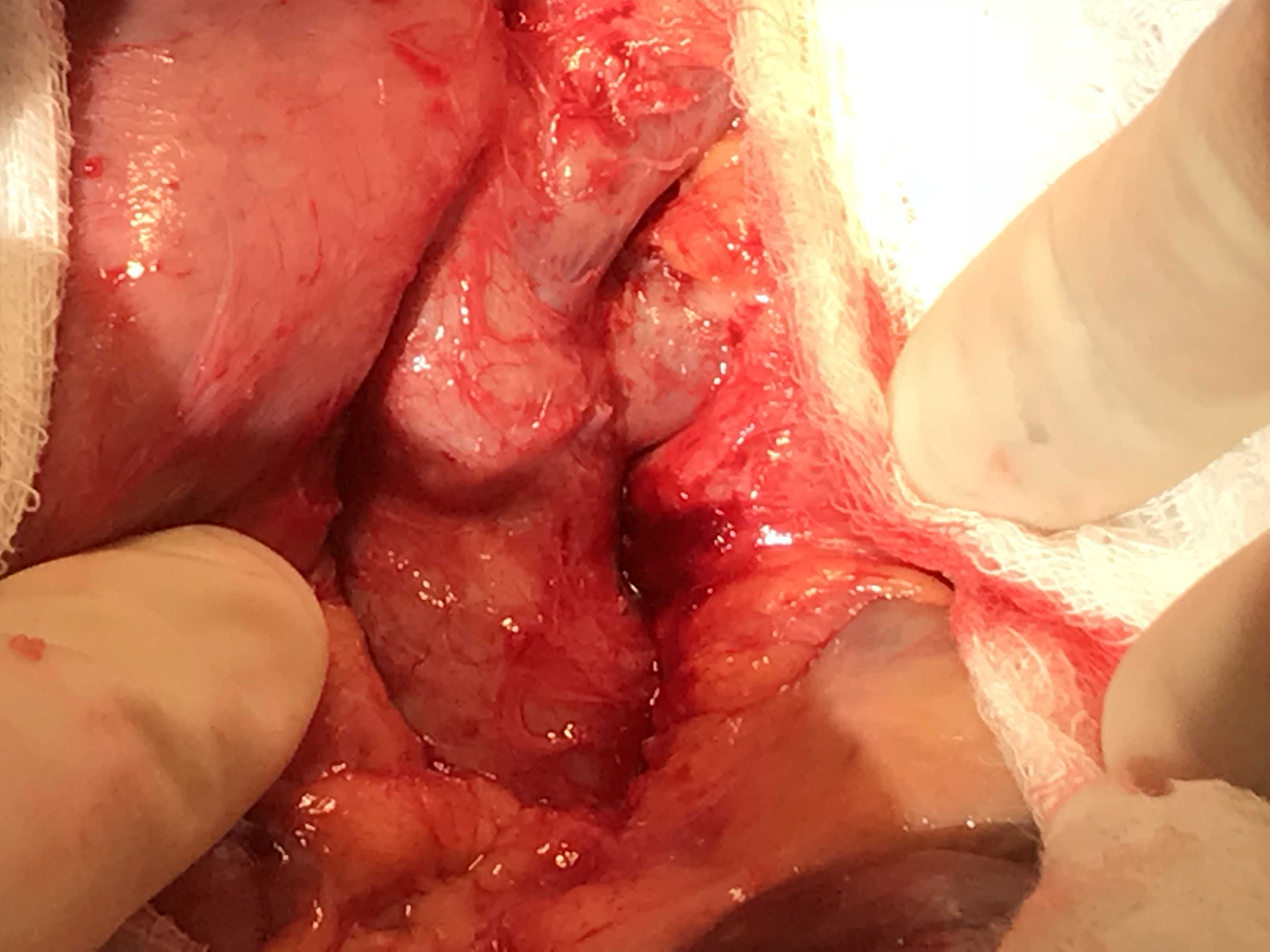
Back to 2019 ePosters