
Nicoladoni-Branham Sign
Denny Scaria, MD MPH, Ramyar Gilani, MD.
Baylor College of Medicine, Houston, TX, USA.
DEMOGRAPHICS
35 year old male
HISTORY
This patient with a history of multiple gunshot wounds to the right groin without any intervention was seen in vascular clinic fourteen years later for several year history of worsening right groin swelling and pulsatile sensation in his groin and thigh. Review of systems was remarkable for numbness and tingling sensation in right leg, dyspnea on exertion and palpitations. Physical exam showed distended veins in the right lower extremity, and for pulsatile mass palpated over the right groin extending to mid medial thigh. Pedal pulses were present. Nicoladoni-Branham sign was present.
PLAN
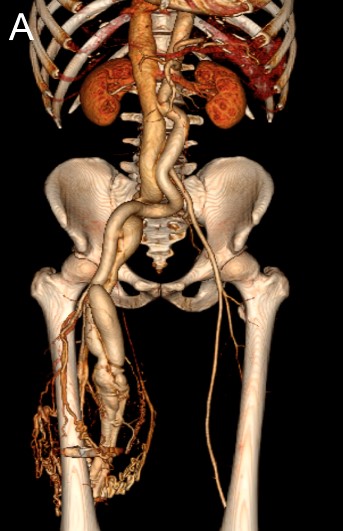
Imaging showed moderate cardiomegaly, a retained bullet in the right thigh, markedly dilated right iliac and femoral arteries, arteriovenous (AV) fistula between the right superficial femoral artery (SFA) and the femoral vein with enlargement of the venous system including the inferior vena cava. Via angiogram, aortocaval fistula was excluded. On exploration an AV fistula was identified between the SFA and femoral vein which was disconnected. Upon clamping the common femoral artery for proximal control, a decrease in heart rate was noted consistent with Nicoladoni-Branham sign elicited in clinic. A large defect was found in the SFA which was primarily repaired, and the vein defect was repaired with a vein patch angioplasty using contralateral greater saphenous vein.
DISCUSSION
Nicoladoni-Branham sign refers to the bradycardia and hypertension noted when the artery proximal to an AV fistula is compressed. It is thought that when the fistula is compressed the afterload abruptly increases resulting in transient hypertension. However, the mechanism of reflexive bradycardia that occurs almost instantaneously is not completely understood. Regardless this phenomenon can be distinguishing for AV fistula thought to be contributing to worsening cardiac function. Although traumatic AV fistulas are well described, description of Nicoladoni-Branham sign indicating hemodynamic significance in association with these fistulas is sparse at best. This case highlights significant long-term sequelae of traumatic AV fistulas and challenges in diagnosis at time of injury for asymptomatic patients.
Back to 2019 ePosters