
False Lumen Fenestrated Endografting to Repair an Aneurysmal Type B Aortic Dissection
Jeniann Yi, David Kuwayama.
University of Colorado, Aurora, CO, USA.
DEMOGRAPHICS: Endovascular treatment of type B aortic dissection (TBAD) traditionally involves aortic true lumen (TL) stent grafting. We describe a case of a fenestrated endograft intentionally deployed in the perivisceral aortic false lumen (FL), with branches deployed to the celiac (CA) and superior mesenteric arteries (SMA).
HISTORY: A 58 year old female with chronic thoracoabdominal TBAD presented with perivisceral FL aneurysmal degeneration. Prior surgery elsewhere included TL thoracic and infrarenal aortic endografting, and bilateral renal debranching. Re-entry tears at the aortic endograft endpoints permitted perivisceral TL and primary false lumen (pFL) access from above and below. Visceral anatomy was complex; the CA originated from a secondary false lumen (sFL), and the prior SMA stent graft crossed TL, ending in pFL.
PLAN: Given her co-morbidities and previous open aortic surgery, a fenestrated endovascular solution was selected. The SMA stent graft mandated pFL deployment of the fenestrated endograft to permit cannulation. However, CA cannulation from the pFL required challenging navigation through an intimal tear, TL, another intimal tear, sFL, into CA orifice. To facilitate CA cannulation, staged repair was performed. In a first operation, stent grafts were deployed from TL across the sFL into the CA. (Figure 1) In a second operation, a fenestrated Cook Zenith TX2 endograft was backtable constructed; one fenestration aligned with the SMA stent graft, and the other aligned with an intimal tear between pFL and TL to access CA. The graft was deployed in pFL, sealing into the prior thoracic and infrarenal endografts. Wire access was established into the SMA stent graft, and a branch deployed. Wire access from celiac fenestration crossed the tear into TL, then into the celiac stents; a branch was then deployed.
DISCUSSION: Although TL stent grafting is standard in endovascular treatment of TBAD, we present a case in which FL endografting was the only fenestrated solution. This strategy is only acceptable if endograft inflow and outflow is known to be TL, and if all visceral targets are easily accessible from the FL. Pre-stenting may be required to achieve these prerequisites. Long term stability of fenestrated endografts deployed in the FL remains uncertain. 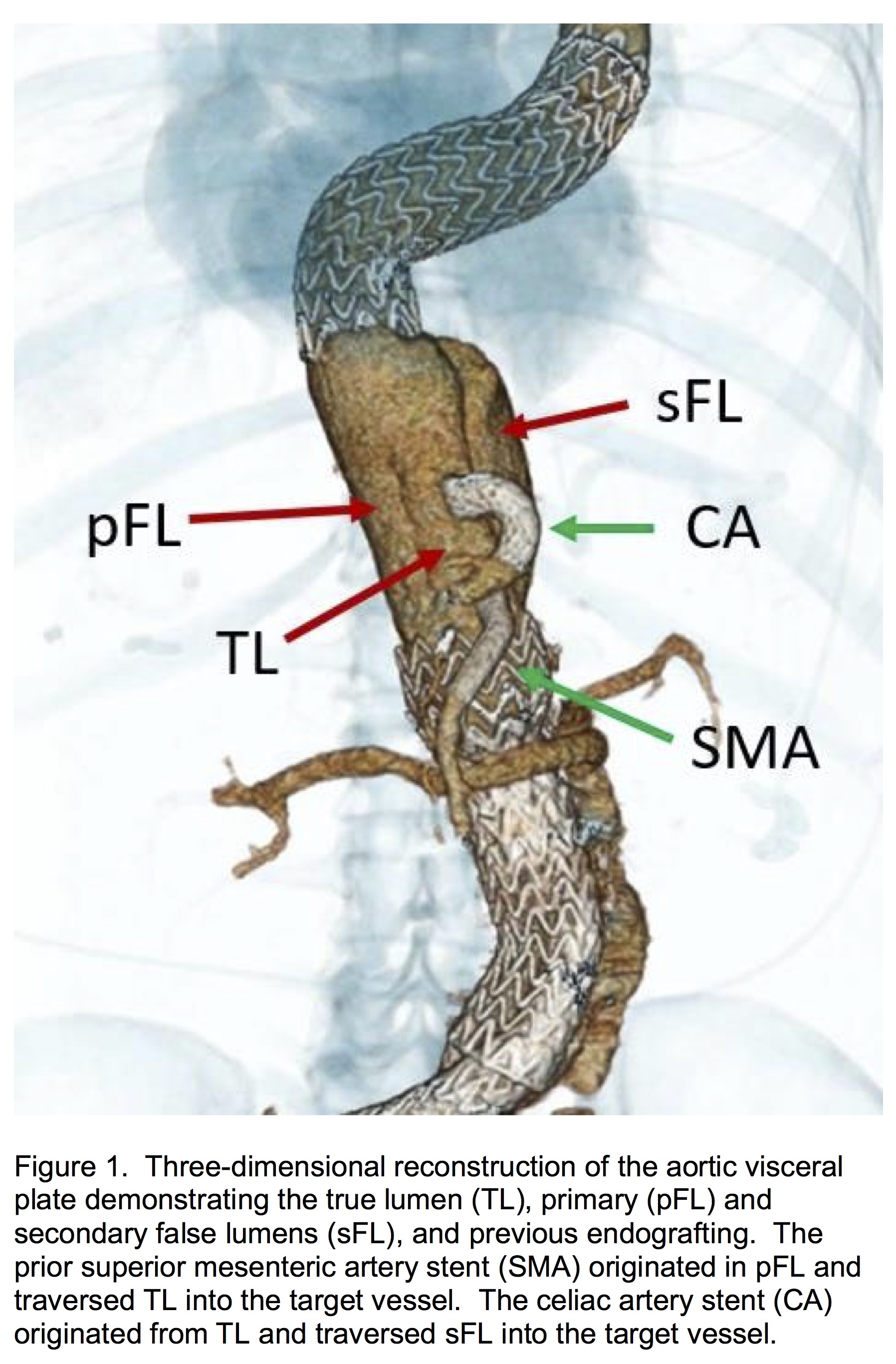
Back to 2019 ePosters