
The role of mediastinoscopy through a supraclavicular incision in the treatment of aberrant right subclavian artery stump
Scott Bendix, MD, Farah Mohammad, MD, Loay Kabbani, MD, Brian Lace, MD.
Henry Ford Hospital, Detroit, MI, USA.
DEMOGRAPHICS: Aberrant right subclavian artery (ARSA) is a rare congenital anomaly. It is usually asymptomatic, however, it can present with symptoms due to compression of the esophagus. Various surgical approaches have been described for the treatment of symptomatic ARSA.
HISTORY: A 61-year-old female presented to our clinic with dysphagia. A CT angiography revealed an ARSA with mass-effect on the esophagus. She described progressive difficulty swallowing solids over the past year and a feeling of “tightness” on the right side of her throat when she swallowed. She was evaluated by gastroenterology, an EGD had been performed that showed no significant pathology. Her presentation was consistent with symptomatic dysphagia lusoria secondary to ARSA.
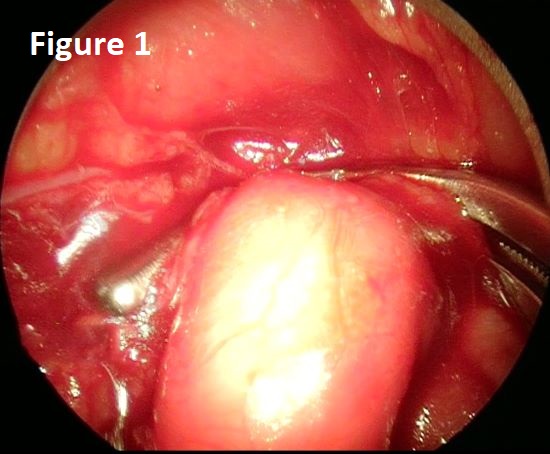
PLAN: The patient was taken to the operating room for right subclavian artery transposition through a supraclavicular approach. The right common carotid artery and the right subclavian artery exposed. A mediastinoscope was inserted through the supraclavicular incision and used to help dissect and mobilize the ARSA under direct vision to its origin off the aorta (figure 1). The right SCA was clamped close to its origin, transected and over-sown. Then a right subclavian to carotid transposition was completed (figure 2). Her post-operative course was uncomplicated. CT angiography prior to discharge showed resolution of the esophageal compression. She was discharged home on post-operative day 3.
DISCUSSION: There are multiple surgical methods described to treat the proximal stump of the ARSA. Options include: open ligation through a sternotomy or thoracotomy, proximal embolization or dissection through a right supraclavicular incision. Approaching the ARSA only through a neck incision is difficult due to the deep origin of the ARSA in the chest. Using a mediastinoscope allowed for the dissection of the ARSA to its origins off the aorta under direct visualization. We believe this approach is a safe and effective modality for treatment of symptomatic ARSA.

Back to 2019 ePosters