
Intravascular Lithotripsy-Assisted BilateralAorto-Iliac Stenting for Calcified Occluded Distal Aorta and Common Iliac Arteries
Courtney Grant, MD, Miguel Montero-Baker, MD, Ramyar Gilani, MD, Joseph Mills, MD, Jayer Chung, MD.
Baylor College of Medicine, Houston, TX, USA.
Demographics: 76-year-old female with history of hypertension, hyperlipidemia, COPD and current tobacco abuse.
History: Bilateral lower extremity rest pain and nonpalpable femoral pulses. CTA revealed a heavily calcified but patent infrarenal aorta and perivisceral aorta. The distal infrarenal aorta and common iliac arteries were chronically occluded. External iliac and infrainguinal vessels were patent but with calcific changes. Right and left ankle brachial indexes were 0.33 and 0.34, respectively.
Plan: Ultrasound-guided retrograde femoral artery access was obtained bilaterally. Diagnostic aortogram via bilateral sheath injection confirmed the severe calcific chronic total occlusion (CTO) of the distal aorta, and bilateral iliac arteries, worse on the left (Figure 1A). An 0.035” angled ZIPwire (Boston Scientific) and Navicross catheter (Terumo) were used to cross the right iliac CTO. Using the same wire and catheter combination, the left iliac lesion was crossed in a subintimal plane, with unsuccessful true-lumen re-entry. An exchange for an 0.014” Spartacore (Abbott) guidewire and performed intravascular ultrasound-guided re-entry (Pioneer, Phillips) into the aortic true lumen. The left iliac CTO was serially dilated with balloons up to 6mm. However, no catheter larger that an 0.014” would cross the lesion. Plaque modification was therefore performed using an intravascular lithoplasty balloon (Shockwave Medical, 4 x 60mm) initially inflated to 6 atm for 90 pulses, then dilated for an additional 120 seconds with lithotripsy (Figure 1B and 1C). This modified the plaque and allowed passage of 7Fr sheaths bilaterally, and subsequent delivery and deployment of bilateral 7 x 59mm balloon expandable covered stents (iCast, Atrium) at the bifurcation in a “kissing” configuration. Completion angiography showed fully-expanded patent iliac stents with excellent flow, without evidence of residual stenosis, dissection, or extravasation (Figure 1D). Palpable pulses were restored with resolution of rest pain.
Discussion: Calcified infrarenal aortoiliac CTO’s represent technical challenges for either open or endovascular repair. Evolving endovascular devices and techniques are permitting increasingly safe and efficacious percutaneous treatment options. To our knowledge, this is the first report of a TASC D calcific aortoiliac CTO successfully modified with intravascular lithoplasty. Further experience with balloon lithoplasty is required to quantify the marginal benefit of this technology. 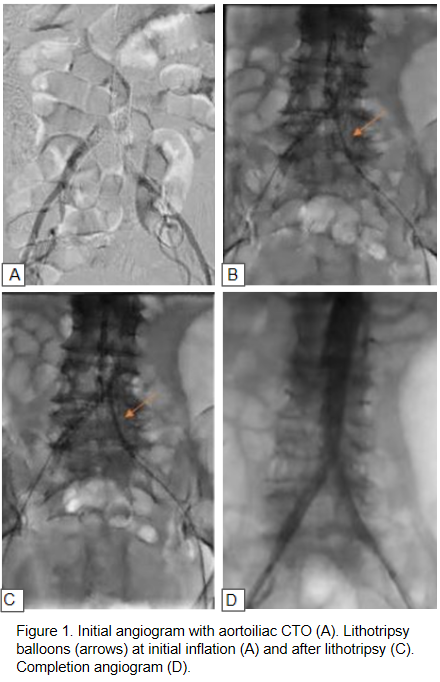
Back to 2019 ePosters