
Novel Utility of Amplatzer Septal Occlusion Device to Treat Persistent Aortocaval Fistula Following Ruptured Endovascular Aortic Aneurysm Repair
Brian Sheehan, MD1, Nii-Kabu Kabutey, MD1, Patrick Lee, MD1, Luke Putnam, MD2, Shelley Maithel, MD2, Ian Gordon, MD, PhD2, Roy M. Fujitani, MD2, Peyman Borghei, MD2.
1University of California, Irvine, Long Beach, CA, USA, 2University of California, Irvine, Orange, CA, USA.
DEMOGRAPHICS: A 68-year-old male presented to the emergency department six months after endovascular aneurysm repair (EVAR) for ruptured abdominal aortic aneurysm (AAA) with one week of shortness of breath, and bilateral lower extremity edema.
HISTORY: The patient’s prior rupture was treated emergently at a community hospital. Upon presentation six months later, echocardiography demonstrated pulmonary and right ventricular hypertension, dilated right ventricle, and an ejection fraction of 55-60%. CT angiography revealed an aortocaval fistula (ACF) (Figure-1a), and type II endoleak.
PLAN: After accessing concomitant right femoral artery and vein, intraoperative aortography confirmed ACF and type II endoleak. The ACF was cannulated, and a 22-mm Amplatzer plug was deployed in the fistula neck followed by coil embolization of the aneurysm sac. Post-embolization aortogram showed persistent ACF, but decreased flow. Due to hemodynamic instability and concern for acute kidney injury, further intervention was deferred. One week later, intraoperative intravascular ultrasound of the inferior vena cava (IVC) revealed a 1-cm fistula neck. Attempted cannulation of the previously embolized aortocaval fistula proved difficult. Thus, the right internal jugular vein was accessed, and the fistula traversed. A 15-mm Amplatzer septal occluder was deployed with the left atrial disc in the aneurysm sac and the right atrial disk in the IVC. Cavogram demonstrated exclusion of the aneurysm sac (Figure-1b). After aortogram revealed delayed filling of the IVC, multiple branches of a prominent right iliolumbar artery feeding the aneurysm sac were embolized (Figure-1c). Final aortogram showed occlusion of the ACF (Figure-1d). The remainder of the patient’s course was uncomplicated.
DISCUSSION: ACF is a potentially fatal sequelae of ruptured AAA. A persistent ACF after EVAR was successfully closed using an Amplatzer septal occluder. The type II endoleaks likely resulted in the pressure gradient responsible for the persistent ACF, and concurrent embolization proved necessary. Two cases in the literature exist regarding use of the Amplatzer device in closure of ACFs, and long-term follow-up is necessary to ensure the durability of repair in this context. The patient has recovered well, and follow up CT angiography demonstrated small persistent type II endoleak. 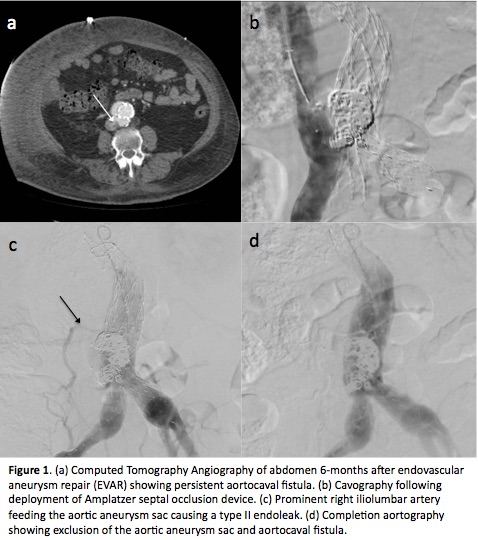
Back to 2019 Abstracts