
On-table Modification of Self-expanding Covered Stents for Hybrid Aortobifemoral Revascularization
Arash Fereydooni, MS1, Chrisitine Deyholos, MD2, Alan Dardik, MD, PhD3, Naiem Nassiri, MD3.
1Yale School of Medicine, New Haven, CT, USA, 2Section of Vascular and Endovascular Surgery, Department of Surgery, Yale University School of Medicine, New Haven, CT, USA, 3VA Connecticut Healthcare System, West Haven, CT, USA.
DEMOGRAPHICS: 72-year-old man with hypertension, hyperlipidemia, 116-pack-year smoking history and chronic obstructive pulmonary disease
HISTORY: He presented with disabling claudication bilaterally, absent lower extremity pulses, and ankle-brachial indices of 0.49 (right) and 0.38 (left). Computed tomography angiography showed: I) left: occlusion of external iliac artery (EIA), nearly occluded calcified common femoral artery (CFA), II) right: diffusely diseased EIA and nearly occluded, calcified CFA, III) patent profunda femoral arteries (PFA) and diseased superficial femoral arteries (SFA) bilaterally with three-vessel run-off.
PLAN: Bilateral CFA endarterectomy with iliac stenting with a novel approach to left EIA revascularization.Bilateral CFAs were surgically exposed. Via left brachial access, a subintimal dissection plane was developed extending into the exposed left CFA. Two Viabahn (Gore, Flagstaff, AZ) covered-stents (7mmx50mm) were deployed from the proximal EIA extending into the mid-CFA and post-dilated. A balloon was insufflated in the stents for proximal control. With the Viabahn stent and wire in place, extensive femoral endarterectomy was performed from distal EIA to proximal PFA (Figure). Next, the anterior surface of the Viabahn stent was cut longitudinally and tacking sutures were placed along the posterior surface of the stent for optimal apposition to the arterial wall. Patch angioplasty was performed, incorporating the surgically modified stent into each bite along the proximal end of the arteriotomy. On the right, traditional femoral endarterectomy and retrograde iliac stenting was performed with deployment of one Viabahn stent in the EIA and one VBX stent in the distal CIA. Completion angiography showed widely patent aortofemoral circulation. Bounding palpable pulses were noted in bilateral legs. Claudication resolved on post-operative day-1. Patient was discharged on day-4. Follow-up ABIs were 1.1 (right) and 0.85 (left).
DISCUSSION: Femoral endarterectomy with iliac stenting is a less invasive alternative to aortobifemoral bypass, but TASC D lesions with contiguous iliofemoral occlusion are challenging for hybrid repair. The technique described here 1) eliminates the need to clamp calcified iliac vessels; 2) allows for better incorporation of iliac stent grafts into endarterectomized plane and smoother transition across the inguinal ligament; and 3) expands the reach of endovascular therapy to chronic total occlusions of iliac vessels. 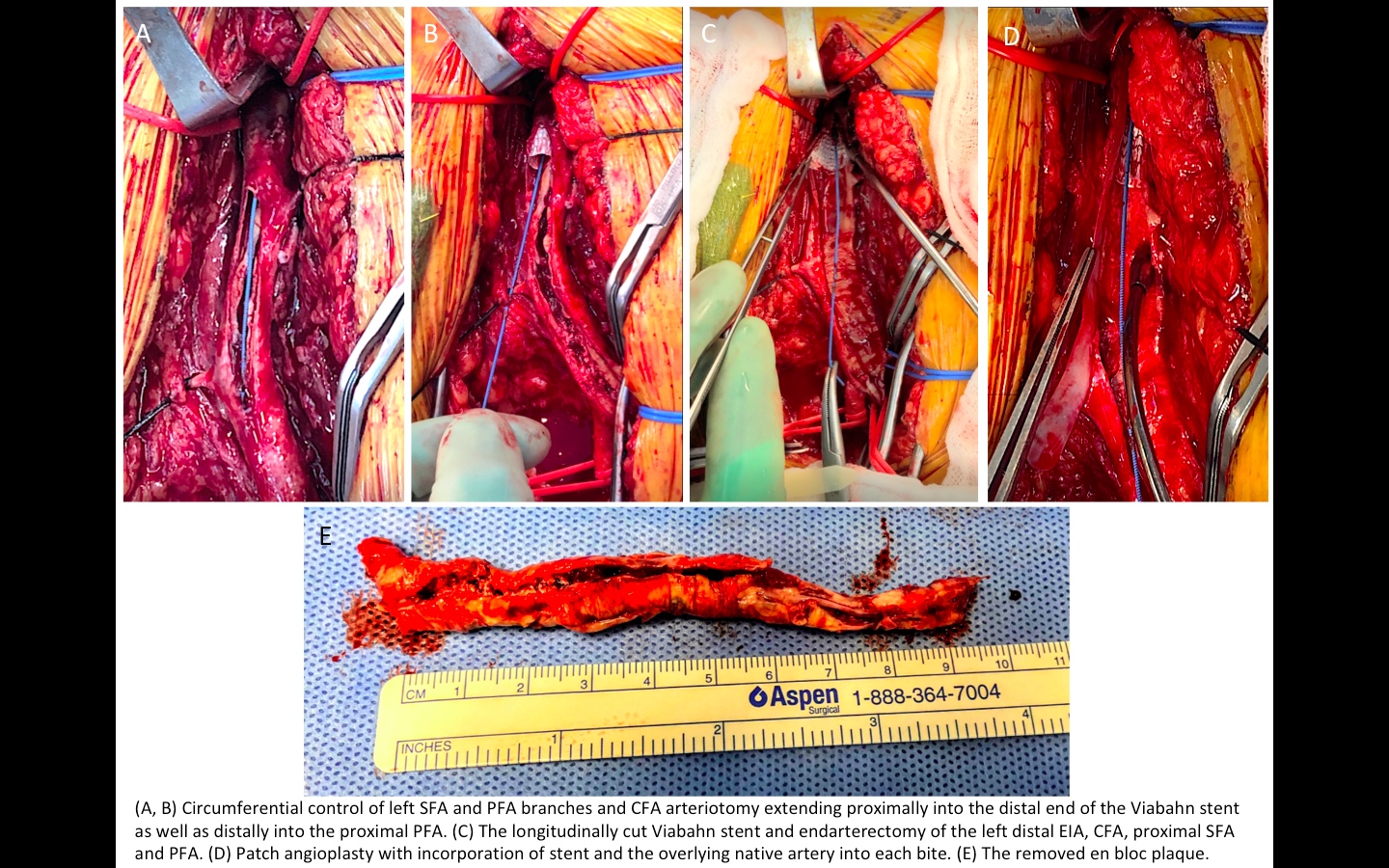
Back to 2019 Abstracts