
Hybrid Revascularization by Transmediastinal Carotid Artery Stenting with Flow Reversal during Coronary Artery Bypass Grafting: A Novel Technique
Zachary F. Williams, MD, Jacob N. Schroder, MD, Mitchell W. Cox, MD, Kevin W. Southerland, MD.
Duke University Medical Center, Durham, NC, USA.
DEMOGRAPHICS: A 72 year old male with a past medical history of tobacco use, hypertension, hyperlidemia, peripheral artery disease, coronary artery disease (CAD), heart failure, and a cerebrovascular accident (CVA). Relevant surgical history is a left carotid endarterectomy (CEA) for symptomatic carotid disease with subsequent restenosis requiring stent placement.
HISTORY: He presented to the ED with angina and dyspnea. He underwent a cardiac catheterization. This revealed three vessel CAD and a left ventricular ejection fraction of 25-30%. He was referred for coronary artery bypass grafting (CABG). Given his prior cerebrovascular disease, a carotid artery duplex and CTA were obtained revealing critical stenosis in the right ICA. PLAN: Given the severity of his carotid disease, he was deemed to be at increased cerebrovascular risk with CABG. Treatment options included: carotid revascularization (CEA, transfemoral carotid stent, or transcarotid stent) prior to CABG, simultaneous carotid and coronary revascularization or CABG followed by carotid revascularization. We recommended simultaneous transcarotid stent with the ENROUTE Transcarotid Neuroprotection and Stent System and CABG. A sternotomy was performed and the left internal mammary artery was harvested. Proximal control of the common carotid artery (CCA) was obtained. The venous sheath was placed in the right femoral vein. The patient was heparinized and the proximal CCA was cannulated. An arteriogram demonstrated a diseased bifurcation and a severe stenosis of the proximal ICA. We exchanged for the arterial sheath. The flow reversal system was connected. Active flow reversal was achieved by clamping the CCA. The lesion was crossed, predilated and stented. The angiographic result was excellent. The sheath was removed, and arteriotomy closed. The cardiac surgery team then performed a three vessel CABG. A Plavix load was given in the operating room at the completion of the case. The patient did well postoperatively without neurologic deficits.
DISCUSSION:
Concomitant coronary and carotid artery disease is a perplexing problem. TCAR via median sternotomy is an attractive option and possible solution. It provides the morbidity benefits of an endovascular strategy while mitigating the risk of stroke by avoiding manipulation of the aortic arch. Further investigation is required prior to widespread adoption of this novel technique. 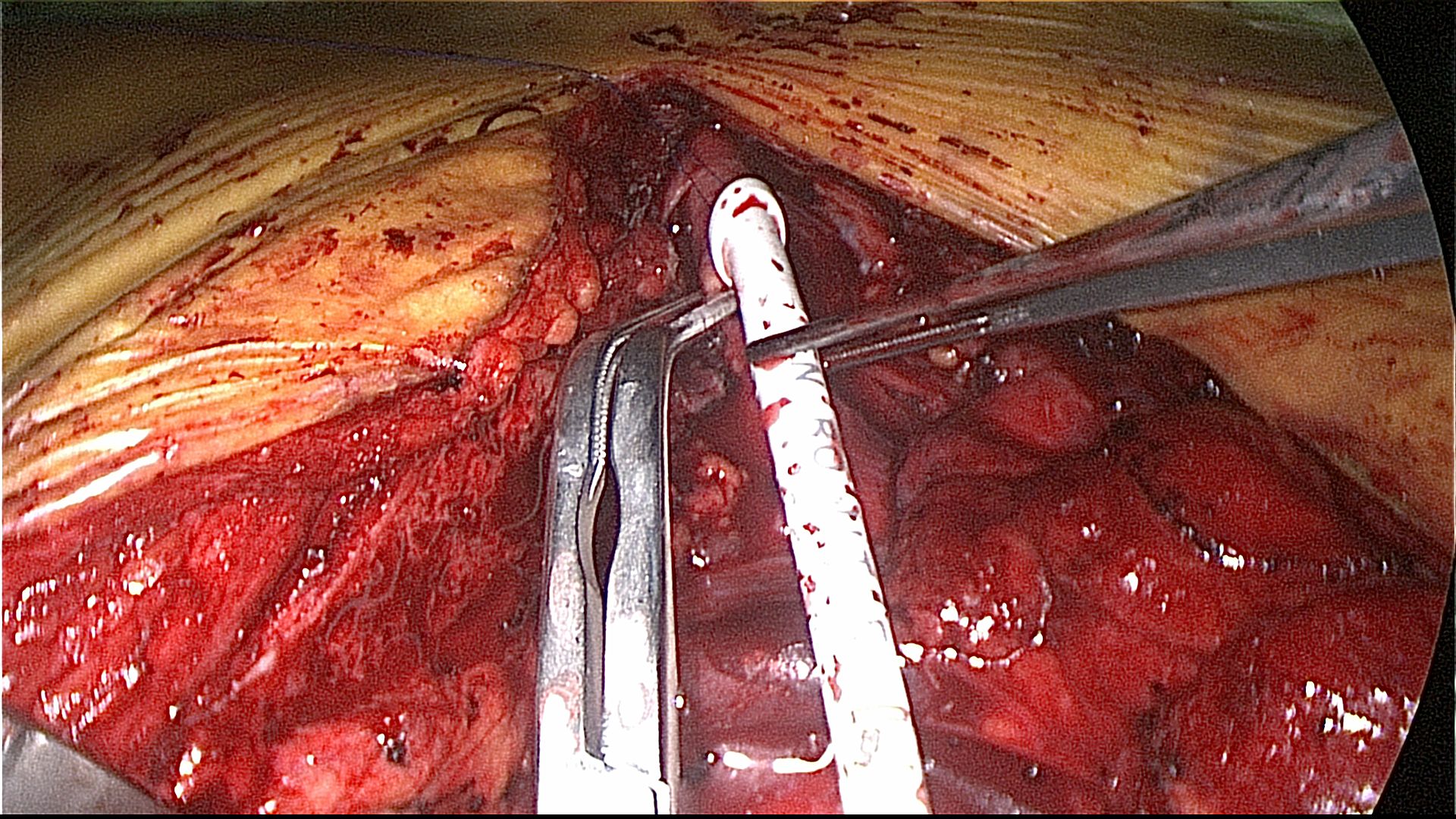
Back to 2019 Abstracts