
Delayed Symptomatic Presentation After Remote Grade 1 Blunt Aortic Injury
Katherine MacCallum, MD, John Futchko, MD, Amit Shah, MD, Aksim G. Rivera, MD.
Jacobi Medical Center/Albert Einstein College of Medicine, Bronx, NY, USA.
OBJECTIVES: Blunt Aortic Injuries (BAI) are the 2ndmost common cause of death after a motor vehicle accident (MVA). The Society of Vascular Surgery (SVS) guidelines recommend endovascular repair of Grade 2-4 BAI after stabilization of all concomitant injuries. However, the management of Grade 1 injuries remains less clear. The current recommendation entails conservative management and serial imaging. Studies have suggested little to no progression of Grade 1 injuries, with some cases even demonstrating resolution of radiographic findings.
METHODS: We report two cases of remote, undiagnosed Grade 1 injury with subsequent symptomatic presentation.
RESULTS:Case 1:51 y/o male with a history of heroin use and previous left parietal stroke presents to ED for treatment of an upper extremity soft tissue infection. Acute onset of blue toes is noted and embolic workup is performed. TEE shows evidence of an intimal flap in the thoracic aorta with associated thrombus and no valvular pathology. CTA shows evidence of intimal tear/flap at the level of the aortic isthmus, as well as embolization to visceral organs. On further questioning he reports a MVA 18 months prior to presentation. He undergoes percutaneous repair with Relay® stent (Bolton, Sunrise, FL). Post-operative course and recovery is uncomplicated.Case 264 y/o male with previous transient ischemic attack, undergoes CT chest for evaluation of pulmonary fibrosis. Findings are significant for spiral intimal tear/flap at the level of the aortic isthmus (Figure 1). Further questioning reveals a fall from a height of 20 feet, 6 years prior to presentation. He undergoes percutaneous repair with a ValiantTMstent (Medtronic, Minneapolis, MN). Post-operative course and recovery is uncomplicated. CONCLUSIONS: Blunt Aortic injuries carry significant mortality and a high index of suspicion should exist in every patient presenting with the appropriate mechanism. Current treatment recommendation for Grade I BAI is conservative management along with serial imaging, for which the timing and interval remain unclear. The delayed presentation of these initially missed injuries suggests that unrecognized minimal aortic injury could further develop into a source of significant morbidity. Targeted prospective studies are needed to further characterize Grade 1 BAI and understand the natural history and progression. 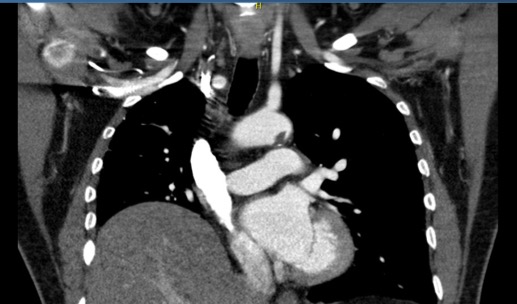
Back to 2019 Abstracts