
Octafen: An Off-the-shelf Configuration For Solving Thoraco-abdominal Aortic Aneurysms
Philip L. Auyang, MD1, Ponraj Chinnadurai, MBBS, MMST2, Jason T. Lee, MD3, Jean Bismuth, MD1.
1Houston Methodist Hospital, HOUSTON, TX, USA, 2SIEMENS MEDICAL SOLUTIONS, Hoffman estates, IL, USA, 3Stanford University Medical Center, Palo Alto, CA, USA.
OBJECTIVES: There are a multitude of endovascular tools and devices under investigation for the treatment of complex visceral aortic aneurysms. Given the varied nature of visceral aortic aneurysms no one single device is commercially available for widespread use today. This poses a particular challenge for practicing vascular surgeons without access to investigational devices. Here we describe how to utilize existing devices that are accessible for vascular surgeons in most clinical settings. We will discuss effective pre-operative planning, illustrate the Octafen endograft configurations, and debate the pitfalls and solutions to each aspect of the build. We aim to contribute to the armamentarium of vascular surgeons at centers that may not have access to investigational fenestrated devices to repair complex aortic pathology in patients that are poor candidates for open aortic repair.
METHODS: This is a retrospective review of seven complex aortic aneurysms repaired at two institutions by utilizing an octopus endograft configuration. We aim to describe the top down build using an off-the-shelf bifurcated EVAR device, visceral stenting in parallel from the docking limb and bilateral renal artery stenting with a customized Zenith fenestrated device for the treatment of type III and type IV thoracoabdominal aortic aneurysms. We will discuss the importance of case planning, specific tips and pitfalls with the described configuration.
RESULTS: Our series experience demonstrated a 100% successful repair rate with no type I or III endoleaks. There were no incidents of acute occlusion of celiac, SMA or renal stents in this series. One gutter endoleak was successfully repaired with coiling of the gutter. Patients required one-night stay in the ICU and were discharged within post-operative day 5. No immediate complications such as paraplegia or rupture were experienced.
CONCLUSIONS: We discuss our in-depth planning for octopus endograft configurations and the successful repair of visceral aortic aneurysms. This configuration has unique challenges that we address. Namely gutter leak is a primary concern, but we utilize available tools and methods for reducing gutter leak. We believe our report will benefit vascular surgeons practicing within a variety of settings to treat complex visceral aortic aneurysms with widely available endovascular tools. 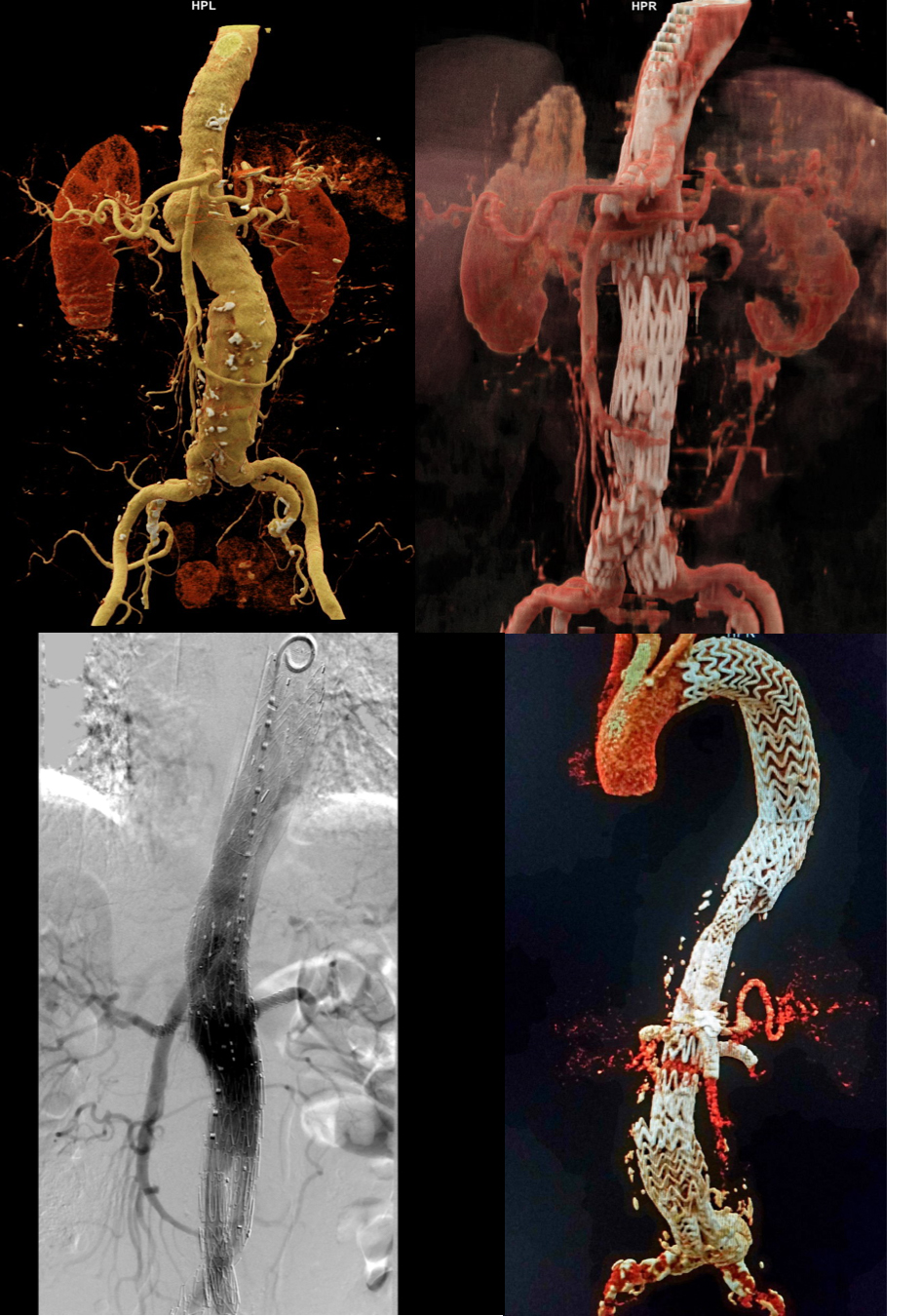
Back to 2020 Karmody Posters