
Treatment And Outcomes Of Aortic Graft Infections: A Single Center Experience
Amanda C. Filiberto, MD, Javariah Fatima, MD, Craig T. Elder, MD, Salvatore T. Scali, MD, Thomas S. Huber, MD, PhD.
University of Florida, Gainesville, FL, USA.
OBJECTIVE: Aortic graft infections (AGI) are both a rare and devastating complication requiring explant of infected prosthesis and complex reconstruction. Despite the variety of methods to treat AGI, there is a paucity of evidence to describe comparative outcomes. Herein, we review surgical management and outcomes of patients with AGI after infrarenal aortic surgery.
METHODS: Study included patients diagnosed with AGI between 2002-2019. Demographics, surgical management and outcomes were extracted via chart review. Primary end-point was mortality and secondary end-points were complications, re-infection, re-intervention and survival.
RESULTS: An AGI was diagnosed in 131 patients (79 males, age 66±10 years). Median time to presentation was 47 months (IQR 13-129 months). Clinical findings at presentation included pain (65%), leukocytosis (54%), fever (22%), and GI bleed (18%). In-situ aortic replacement was performed in 86 patients (66%) using neoartoiliac system in 44 (34%), PTFE in 33 (25%), cryopreserved-allograft in 31 (24%), and Dacron in 25 (19%). Extra-anatomic axillo-femoral-bypass was performed in 33 patients (25%). An aortoenteric-fistula was noted in 39 (30%) patients. Blood cultures were positive in 20 of 93 (22%) obtained on admission. Staphylococcus aureus was the most commonly isolated organism. Thirteen (11%) patients were prescribed lifelong antibiotics postoperatively. Excluding lifelong antibiotics, mean postoperative antibiotic duration was 41±24 days. Median follow up was 3 months (IQR 1-16 months). In-hospital/30-day mortality was 19%. There was one intraoperative death. The most common major complication was respiratory failure in 22%, followed by acute kidney injury in 15%. Overall 1-year and 5-year survival were 68±4% and 51±5%, freedom from re-infection at 1 year and 5 years was 91±3% and 69±10%, freedom from re-intervention at 1 year and 4 years was 87±4% and 72±9%, freedom from major adverse limb event at 1 year and 4 years was 80±5 % and 69±10%, and primary patency at 1 year and 4 years was 87±4 % and 80±7%, respectively (Figure 1).
CONCLUSIONS: Aortic graft infection results in significant early morbidity and mortality with surgical extirpation; however, late term survival is good in appropriately selected patients. The risk of late re-infection mandates lifelong surveillance and consideration of indefinite anti-microbial suppression. 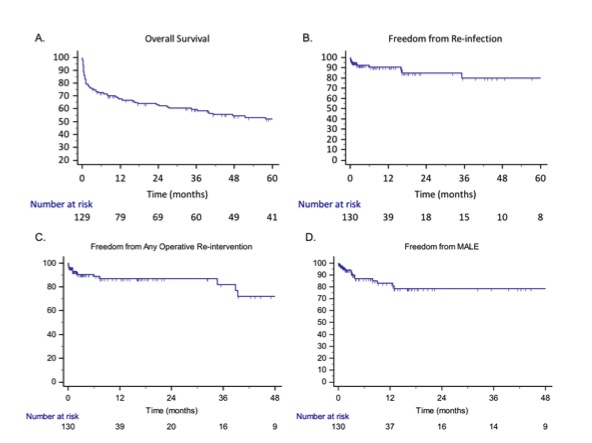
Back to 2020 Karmody Posters