
Defining Expected Surveillance Duplex Ultrasound Results In Distal Revascularization And Interval Ligation Conduits
Alexis Graham, MD1, M Libby Weaver, MD1, Courtenay Holscher, MD PhD1, Thomas Reifsnyder, MD2.
1Johns Hopkins Hospital, Baltimore, MD, USA, 2Johns Hopkins Hospital Bayview, Baltimore, MD, USA.
OBJECTIVES: The SVS has practice guidelines regarding follow-up after arterial procedures, including duplex ultrasound findings. However, there is limited literature on expected duplex findings following distal revascularization and interval ligation (DRIL) procedures. This study evaluated the duplex ultrasound characteristics and the hemodynamic results of DRIL. METHODS: A retrospective chart review of patients who underwent DRIL between 2008-2019 was performed. Patients without both preoperative and follow-up data containing imaging, finger pressures (FP), or wrist brachial index (WBI) were excluded. Hemodynamic results were assessed using a paired t-test. RESULTS: Of 72 patients undergoing DRIL, 38 met inclusion criteria. All DRILs utilized autogenous conduits. Median time to first follow up (fFU) was 23 days (range 1-225d) where 12 had complete resolution of their symptoms and 26 had partial resolution. Of the 27 patients that had pre- and post-operative WBIs and FPs, there was a significant improvement (p<0.001) with the median WBI increasing from 0.56 to 0.90 and the median finger pressure improving from 56 to 73. 25 patients had a second follow up (sFU) with median time from DRIL of 118d (range 11-843d). There was no significant difference in WBI or FP between fFU and sFU. During fFU, the median duplex ultrasound velocities of the DRIL conduit were high proximally (inflow 235cm/s, proximal anastomosis 217.7cm/s) but slowed distally (mid-conduit 46.4cm/s, distal anastomosis 78.3cm/s, outflow 59.3cm/s). The same pattern of velocities held constant at the sFU. CONCLUSIONS: DRIL is an effective treatment for access related ischemia as confirmed by significantly increased distal pressures. This study is the first to demonstrate the unique duplex characteristics of a DRIL. The typical velocities at the proximal anastomosis are significantly elevated without evidence of stenosis while the velocities in the main body and distal aspects are what would be expected in a resting upper extremity. We suspect the elevated velocities at the proximal anastomosis are due to the rapid flows in the brachial artery which feeds both the DRIL and the fistula. Therefore, elevated velocities at the proximal anastomosis do not necessarily warrant further evaluation without other evidence of conduit compromise. 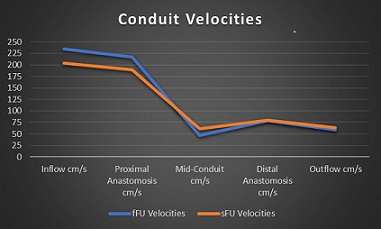
Back to 2020 Karmody Posters