
Aortic Neck Dilatation Following Endovascular Repair Of Thoracic Aortic Aneurysm
Patricia O. Yau, MD1, Patricia Friedmann, MS2, Jeffrey Indes, MD1, Evan Lipsitz, MD, MBA1, Hasan Aldailami, MD1.
1Montefiore Medical Center, Bronx, NY, USA, 2Albert Einstein College of Medicine, Bronx, NY, USA.
Objective: Thoracic endovascular aortic repair (TEVAR) has become a mainstay of treatment for thoracic aortic aneurysm. Expansion of the proximal aortic neck after endovascular repair of abdominal aortic aneurysms has been demonstrated; however, dilatation of the proximal aortic neck after TEVAR has not been well described. We sought to describe remodeling of the proximal neck following TEVAR for thoracic aortic aneurysm.
Methods: This is a retrospective review of patients who underwent TEVAR for thoracic aortic aneurysm at a single institution from 2010-2018. Postoperative computed tomography (CT) scans were reviewed and aortic diameter was measured in orthogonal planes using 3-dimensional centerline reconstruction software, at four predetermined sites relative to the proximal extent of the graft: at the proximal extent of the graft (Na), 5 mm distal (Nb), 20 mm proximal (PNa), and 10 mm proximal (PNb). The primary outcome was change in aortic diameter as compared to the initial postoperative CT scan. Clinical and operative data were analyzed to identify factors associated with significant neck dilatation.
Results: Twenty-five patients underwent TEVAR for thoracic aortic aneurysm and had sufficient postoperative imaging, with median follow up of 21 months (range: 6-64). Median age was 62 years, and 12 patients (48%) were female. All four sites experienced a mean increase over time in aortic diameter. Of the four sites, Nb had the greatest rate of neck expansion, with median increase of 1.5 mm (IQR, -0.1-3.5) at one year, 2.9 mm (IQR, 0.8-7.2) at two years, and 6.7 mm (IQR, 4.3-8.6) at three years. When comparing patients who had significant neck expansion at Nb (mean rate > 2.0 mm/year) with patients who did not (mean rate < 2.0 mm/year), a higher percentage were smokers (100% vs. 43.8%, p=0.0078), and had a history of COPD (44.4% vs. 6.3%, p=0.04).
Conclusions: Aortic neck dilatation occurs over time for the majority of patients following TEVAR for thoracic aortic aneurysm, with the distal neck experiencing the highest rate of expansion. Smoking and COPD were found to be associated with a higher rate of neck dilatation. 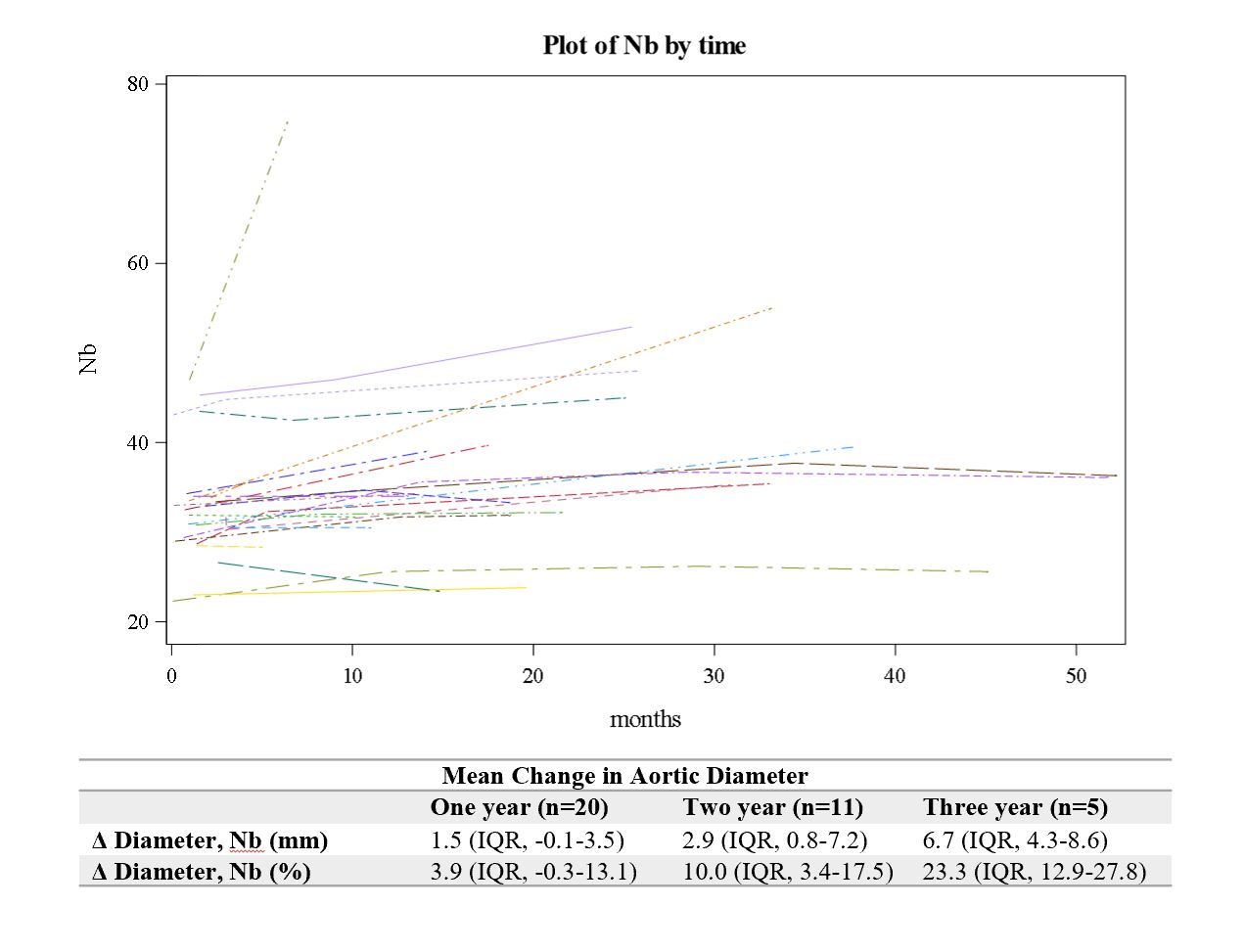
Back to 2020 Karmody Posters