
Open Inferior Vena Cava Filter Removal
Danon Garrido, MD, Miguel Viallobos, MD, Fred Rushton, MD, Marc E. Mitchell.
University of Mississippi Medical Center, Jackson, MS, USA.
OBJECTIVES: The last several decades have seen dramatic changes in the standards for both the insertion and removal of inferior vena cava (IVC) filters. Retrievable and non-retrievable IVC filters can frequently be removed using endovascular techniques. Since IVC filters rarely cause symptoms or result in complications, those that cannot be easily remove are usually left in place. Open removal is reserved for IVC filters with complications or causing symptoms that cannot be removed using endovascular techniques.
METHODS: The results of open IVC filter removal at a single academic medical center from January 2011 through June 2019 were reviewed.
RESULTS: Nine open IVC filter removals were performed. Six (68%) patients were female. The mean age was 46 years (range 26 - 65 years). The filters had been in place for a mean of 6.6 years (range 1 to 12 years). Six (68%) of the filters were originally placed because of deep venous thrombosis with pulmonary embolus in patients with contraindications to anticoagulation. Three (33%) were placed prophylactically in high risk trauma patients not able to be anticoagulated. The most common indication for IVC filter removal was severe malposition of the filter with filter erosion through the IVC wall (n=4) (Figure). Other indications included chronic back pain with filter struts eroding into vertebral bodies (n=3) and strut erosion into the duodenum (n=2). The mean length of stay was 6 days (range 4 - 16 days). Complications included one post-operative ileus and two wound complications, one requiring reoperation. In seven (78%) cases, the filer was captured through a small venotomy after mobilization of the vena cava and cutting the protruding struts. Two patients required an extensive venotomy to remove the filter. Only one of the three patients with back pain had symptom resolution.
CONCLUSIONS: IVC filters that cannot be removed using endovascular techniques, can be safely removed with an open procedure. In most patients, the filter can be captured and removed through a small venotomy; an extensive venotomy is not usually required. The majority of patients with back pain do not have relief of symptoms following IVC filter removal. 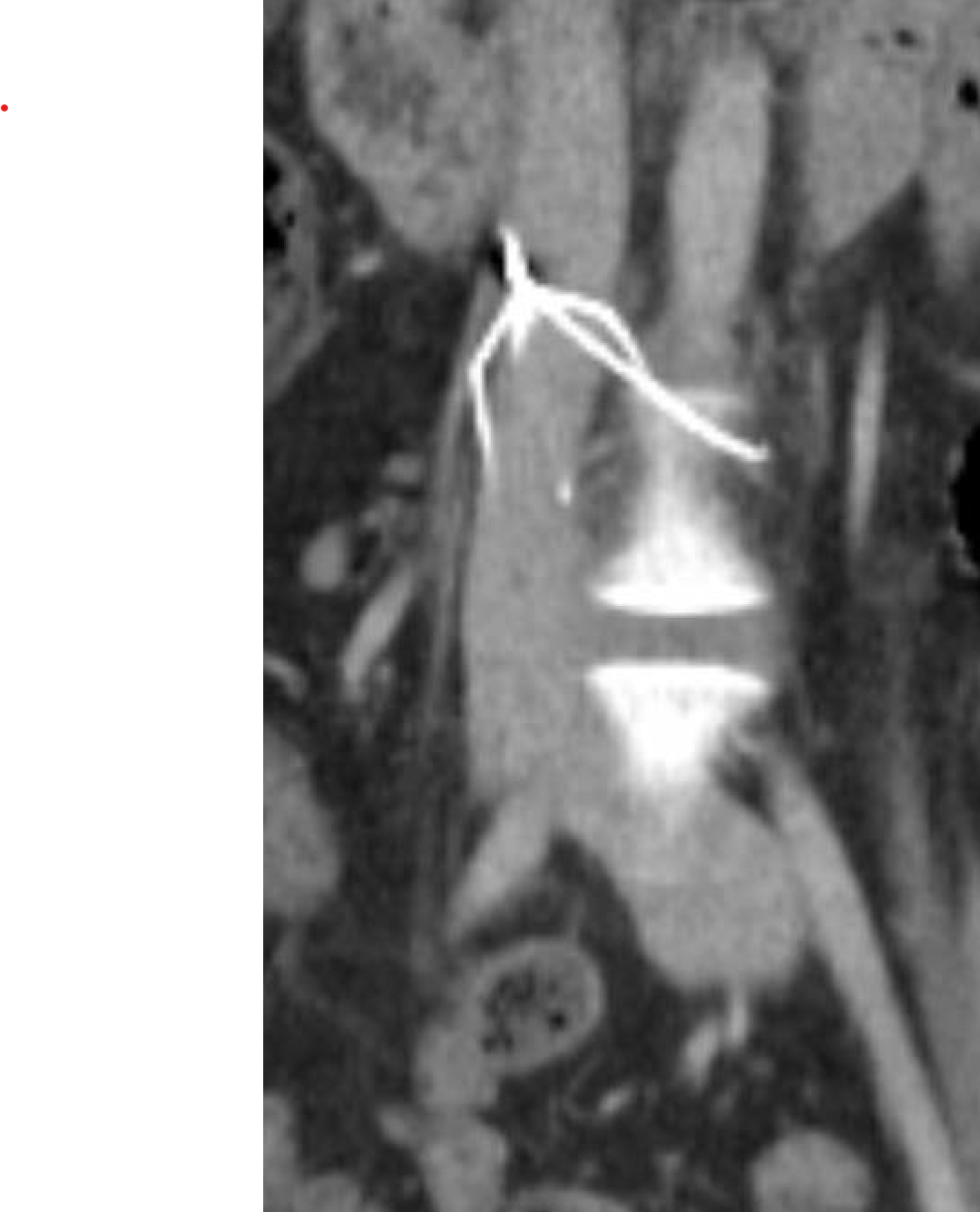
Back to 2020 Abstracts