
The Hyperattenuating Crescent Sign Is Not A Sign Of Impending Rupture
Jordan B. Stoecker, MD, Kevin C. Eddinger, MD, Alison M. Pouch, PhD, Paul J. Foley, III, MD, Grace J. Wang, MD, Ronald M. Fairman, MD, Benjamin M. Jackson, MD.
Hospital of the University of Pennsylvania, Philadelphia, PA, USA.
OBJECTIVE: The "crescent sign" is a hyperattenuating crescent-shaped region on CT within the mural thrombus or wall of an aortic aneurysm. Although it has previously been associated with aneurysm instability or impending rupture, the literature is largely based on retrospective analyses of urgently repaired aneurysms. We strove to more rigorously assess this association by reviewing all patients at our institution with crescent signs.
METHODS: Patients were identified by querying a single institutional PACS database for radiology reports noting a crescent sign. Adult patients with a CT demonstrating a descending thoracic, thoracoabdominal, or abdominal aortic aneurysm and crescent sign between 2004 and 2018 were included. All data expressed as mean ± standard deviation unless noted.
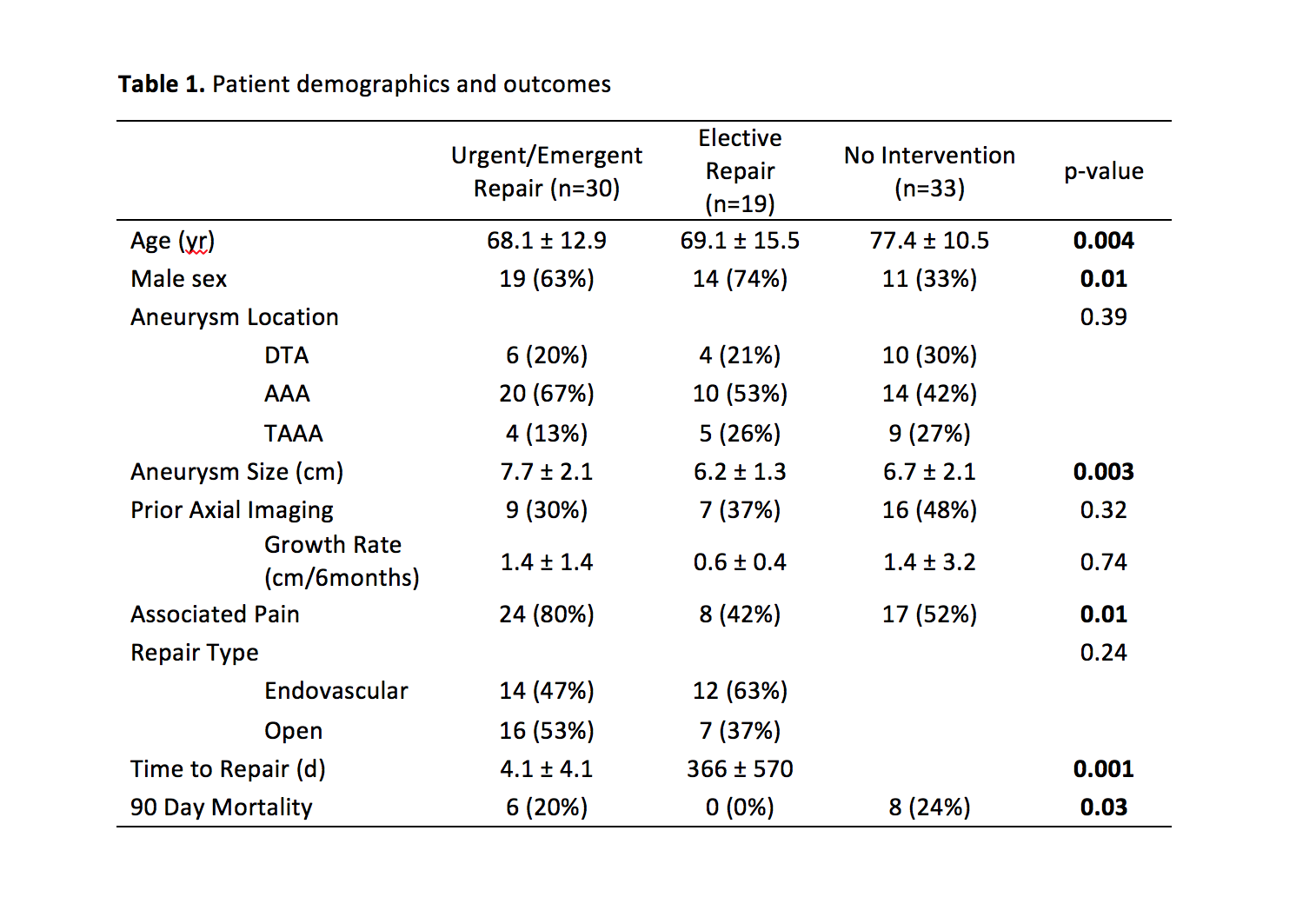
RESULTS: A total of 82 patients were identified. Aneurysm size was 7.1 ± 2.0 cm. Patient demographics are listed in Table 1. There were 32 patients with prior axial imaging within 2 years. Among those patients, mean aneurysm growth rate was 1.2 ± 2.4 cm per 6 months. Thirty patients had emergent or urgent repairs during their index admission (37%), 19 had elective repairs at a later date (23%), and thirty-three patients had no intervention due to either patient choice or prohibitive medical comorbidities (40%). Patients without intervention had a median follow up of 275 days before death or loss to follow up. One patient with an 8.1 cm aneurysm planned for urgent repair experienced acute rupture before transfer to the operating room and expired after endovascular repair. In patients undergoing elective intervention, 6,968 patient-days elapsed between presentation and repair, with zero episodes of acute rupture (median 105 days). These patients had smaller aneurysms compared to those who underwent emergent/urgent repair (6.2 cm vs 8.0 cm, p=0.002) and lower 90-day mortality (0% vs 20%, p=0.04). No surgical candidate with an aneurysm smaller than 8 cm ruptured.
CONCLUSIONS: These findings indicate that a crescent sign on CT in asymptomatic patients with small aneurysms more likely reflects rapid aneurysmal growth than imminent rupture. Elective repair is acceptable in asymptomatic patients with a crescent sign and small aneurysms can be safely observed in the setting of a crescent sign.
Back to 2020 Abstracts