
Selective Fenestration Of IMA Using Physician Modified Endografts To Expand The IFU Of EVAR In Patients With Selective Mesenteric Ischemia
Amarseen Mikael, MD1, Ann Yufa2, Iden Andacheh, MD1.
1UC Riverside SOM/Riverside Community Hospital, Riverside, CA, USA, 2UC Riverside SOM, Riverside, CA, USA.
DEMOGRAPHICS: Current instructions for use (IFU) for endovascular aortic repair (EVAR) prohibit the use of the endograft in the setting of mesenteric atherosclerotic disease with a large patent inferior mesenteric artery (IMA). Studies have shown that up to 18% of patients older than 65 have significant stenosis or occlusion of either the superior mesenteric artery (SMA) or celiac artery without any apparent symptoms due to collateral flow. We present a unique case of a physician-modified endograft for a 5.8 cm abdominal aortic aneurysm (AAA) necessitating an IMA fenestration due to an occluded SMA. Cases such as this may serve to push the current IFU limitations for EVAR.
HISTORY: A 71 year-old male with history of coronary artery bypass grafting and chronic obstructive pulmonary disease was referred for a 5.8 cm AAA. The patient was not a candidate for standard EVAR given that he was found to have an occluded SMA on computed tomography angiogram (CTA). Moreover, the patient was also found to have a 6 mm IMA. Prior attempts at recanalization of the SMA were unsuccessful. It was noted that the bilateral hypogastric arteries were also occluded. In addition to the bowel, the IMA appeared to be the principal blood supply to the pelvis.
PLAN: Given the patient’s comorbidities, he was deemed a high-risk candidate for open repair. A physician-modified fenestrated endovascular aneurysm repair (f-EVAR) with selective fenestration and stenting of the IMA was recommended. Modification was performed on 32 mm by 109 mm Cook Alpha device. The IMA was stented using a 6 mm x 29 mm balloon-expandable Viabahn stent. Post-operative course was not complicated, and he was discharged home on day 2. CT imaging at 3 months post-op showed complete thrombosis of the sac with preserved flow through visceral stents.
DISCUSSION: Only one case of f-EVAR with fenestration of the IMA has previously been reported. However, we present the first case in which the SMA is also occluded. Our case demonstrates that f-EVAR may serve as an option for select patients who do not meet IFU for standard EVAR due to mesenteric atherosclerotic disease. 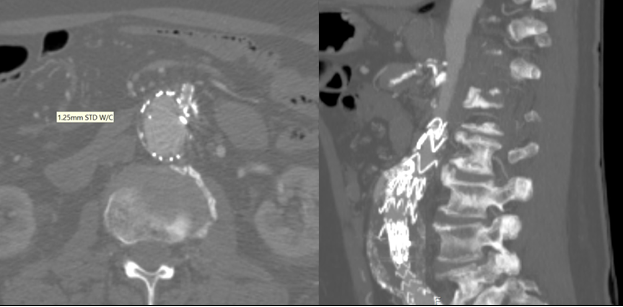
Back to 2020 Abstracts