
Femoral Endarterectomy Is Effective For Claudication And Rest Pain But Not Tissue Loss
Abhisekh Mohapatra, MD, MS, Karim M. Salem, MD, Bowen Xie, MD, Yash K. Pandya, BS, Steven A. Leers, MD, Michel S. Makaroun, MD, Efthymios D. Avgerinos, MD, Eric S. Hager, MD.
University of Pittsburgh Medical Center, Pittsburgh, PA, USA.
OBJECTIVES: Outcomes of femoral endarterectomy (FEA) are poorly described, especially in patients with critical limb ischemia. We sought to examine perioperative and longer-term outcomes after FEA.
METHODS: Retrospective review of patients undergoing elective FEA from 2013-2015 was performed. Patients were included if they underwent concomitant endovascular intervention but not concomitant bypass. The primary outcome was clinical improvement in Rutherford classification (improvement or resolution of claudication or rest pain, or healing of the index wound) within six months and without secondary interventions.
RESULTS: A total of 231 limbs were included with indications of claudication (34.6%), rest pain (27.7%), or tissue loss (37.7%). TransAtlantic InterSocietal Classification (TASC) II C/D iliac and femoropopliteal disease were noted in 15.2% and 46.7%, respectively; retrograde iliac stenting was performed in 27.7% and antegrade femoropopliteal stenting in 9.5%. On completion, all patients had a patent aortoiliac segment but 40.5% had occluded femoropopliteal arteries and relied on profunda femoris outflow; femoropopliteal occlusion was more common with tissue loss (55.4%) than with rest pain (42.6%) or claudication (19.7%; P < .001). Thirty-day mortality was 3.5% and incisional complications (19.1%, including 7.4% surgical site infection) were particularly common. Rutherford classification improved in 80.4% and was significantly more common with a patent femoropopliteal segment (85.6% vs. 68.8%, P = .007) and with claudication or rest pain than with tissue loss (100% vs. 93.3% vs. 49.3%; P < .001). Kaplan-Meier estimated freedom from reintervention (Figure) was lower in patients with tissue loss (50.4% at four years) compared to those with claudication (75.4%) or rest pain (71.2%; P = .0002) and was also lower in patients with an occluded femoropopliteal segment (57.6% vs. 67.7% at four years, P = .04). Complete wound healing within six months was achieved in 61.8% of patients with a patent femoropopliteal segment and 26.6% of patients with femoropopliteal occlusion (P = .0003).
CONCLUSIONS: FEA is an effective and durable treatment in patients with claudication or rest pain. Patients with tissue loss, especially those with an occluded femoropopliteal segment, often require secondary interventions and may be better served with more extensive revascularization as their initial therapy. 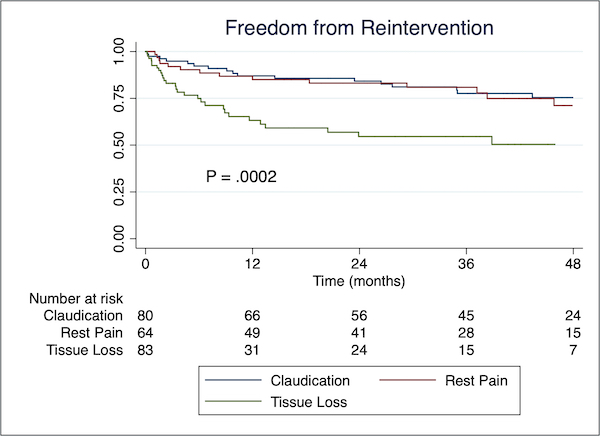
Back to 2020 ePosters