
Effect Of Chronic Kidney Disease On 30 Day Outcomes For Repair Of Complex Abdominal Aneurysm
Denzel R. Woode, MD1, Ambar Mehta, MD1, Christopher A. Latz, MD2, Marc L. Schermerhorn, MD, FACS3, Samuel I. Schwartz, MD2, Danielle R. Bajakian, MD1, Richard Schutzer, MD1, Hiroo Takayama, MD, PHD1, Virendra I. Patel, MD, MPH1.
1New York Presbyterian/Columbia University Medical Center, New York, NY, USA, 2Massachusetts General Hospital, Boston, MA, USA, 3Beth Isreal Deaconess Medical Center, Boston, MA, USA.
Objective:
Chronic kidney disease (CKD) has been shown to increase morbidity and mortality after repair of infrarenal aortic abdominal aneurysm (AAA) and negatively impacts long term survival of patients undergoing aneurysm repair. This study further analyzes the association of CKD severity on the peri-operative outcomes of open (OaR) and fenestrated (FEVAR) repair of complex abdominal aortic aneurysm repair (cAAA) (juxtarenal, suprarenal, and supra visceral AAA).
Methods:
The National Surgery Quality Improvement Program (NSQIP) database was queried by Current Procedural Terminology code (CPT) to identify patients who had undergone OaR or FEVAR for non-ruptured cAAA Jan 2005 to Dec 2016. Patients were stratified by mild (class 1 or 2), moderate (class 3), or severe (class 4 or 5) CKD. Univariate and multivariate analysis were used to compare the demographics, preoperative characteristics, and perioperative outcomes of each group.
Results:
A total of 3662 patients were identified, with 1165 having undergone FEVAR, and 2497 having undergone OaR. Mild, moderate, and severe CKD were found in 66%, 30%, 3.4% of patients, respectively. A 30-day mortality of 4.1%, 7.1%, and 14% (p value: <.0001) was observed in patients with mild, moderate, and severe CKD, respectively. Severity of CKD (mild, moderate, severe) was associated with increase in length of hospital stay (8.1, 9.5, 12 days, p-value: <.0001), renal complications, (5.1%, 11%, 18% p-value: <.0001), pulmonary complications (13%, 18%, 26% p-value: <.0001), and cardiac complications (3.9%, 6.0%, 8.7%, p-value: <.0001). On multivariable risk adjusted analysis, severe CKD was significantly (p<0.05) associated with risk of mortality (OR 2.3 [95%CI 1.3-4.2]) (Table 1), all complications (OR 3.1 [95%CI 2.0-4.9]), and renal complications (OR 3.5 [95%CI 2.1-5.8]). Moderate CKD was significantly associated with risk of mortality (OR 1.5 [95%CI 1.1-2.0]) (Table 1), risk of all complications (OR 1.2 [95%CI 1.1 - 1.5]) and renal complications (OR 2.3 [95% CI 1.8-3.0]).
Conclusion:
This study shows that there is a significant association with increasing severity of CKD and increasing mortality and morbidity post-operatively after repair of cAAA. This data suggests that elective repair of cAAA in patients with severe CKD should be re-considered, due to the significantly elevated operative risks. 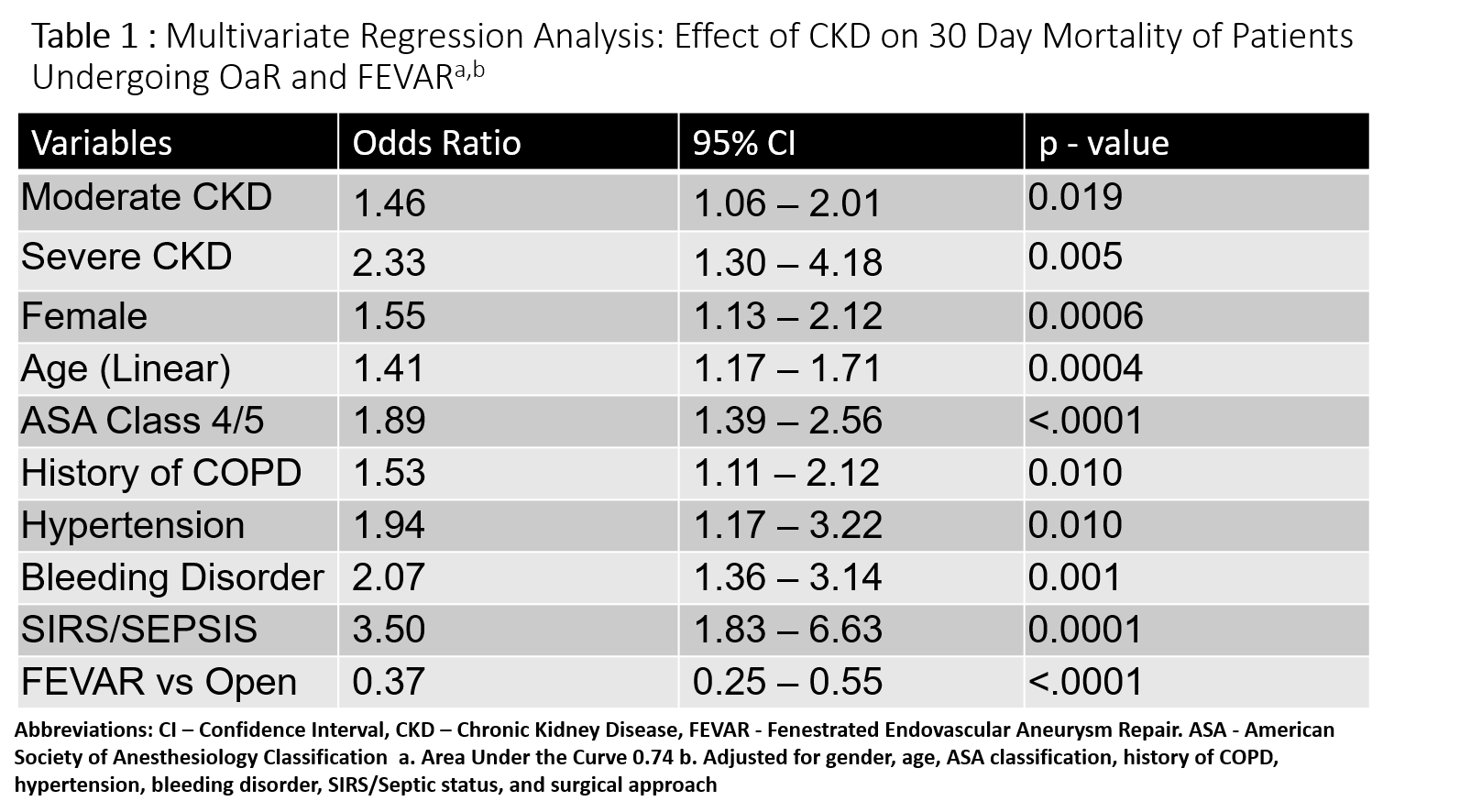
Back to 2020 ePosters