
Variation In Timing Of Guideline-driven Preventative Measures In Patients With Diabetes And Peripheral Arterial Disease
J. Aaron Barnes, MD1, Mark A. Eid, MD1, Zachary J. Wanken, MD, MS1, Richard J. Powell, MD1, David H. Stone, MD1, Barbara Gladders, MS2, Mark A. Creager, MD1, Philip P. Goodney, MD, MS1.
1Dartmouth-Hithcock Medical Center, Lebanon, NH, USA, 2The Dartmouth Institute for Health Policy and Clinical Practice, Lebanon, NH, USA.
OBJECTIVES: Patients with diabetes and peripheral arterial disease (PAD) are at high risk for amputation. Guideline-driven preventative measures for diabetes and PAD, defined as hemoglobin A1c testing (HA1c), diabetic foot care, and vascular assessment, have been shown to be widely effective in limiting amputation risks, even among high risk patients. This study examines the regional variation in the use of guideline-driven preventative measures in patients recently diagnosed with both diabetes and PAD.
METHODS: All Medicare claims from January 2003 until December 2016 were queried using previously validated diagnosis codes to identify patients with newly diagnosed concomitant diabetes and PAD. We identified the time required from the diagnosis of diabetes and PAD to receive each of these guideline-driven preventative measures. We then examined the proportion of patients who received these measures in the first 6 months after diagnosis of diabetes and PAD, as well as regional variation in the use of these measures overall.
RESULTS: Over the study period, 10,506,254 Medicare beneficiaries with concomitant diagnoses of diabetes and PAD were identified. Across all patients, the mean time required for a patient to receive an HA1c test was 259 days, which was shorter than the 440 days for vascular imaging and 499 days for diabetic foot exam, albeit this later measure was coded unreliably. Within the first 6 months of diabetes and PAD diagnosis, there was a 5-fold difference in rate of first foot exam and a 2-fold difference in rate of first vascular assessment across HRRs (Figure). Rates of first HA1c testing demonstrated the least variation across HRRs (range: 40.5% - 63.5%).
CONCLUSIONS: Significant regional variation exists in rates of testing within 6 months of diagnosis with concomitant diabetes and PAD among Medicare patients, and testing rates are low in many regions. Efforts should focus on earlier and more consistent implementation of guideline-driven preventative measures in this high-risk patient population. 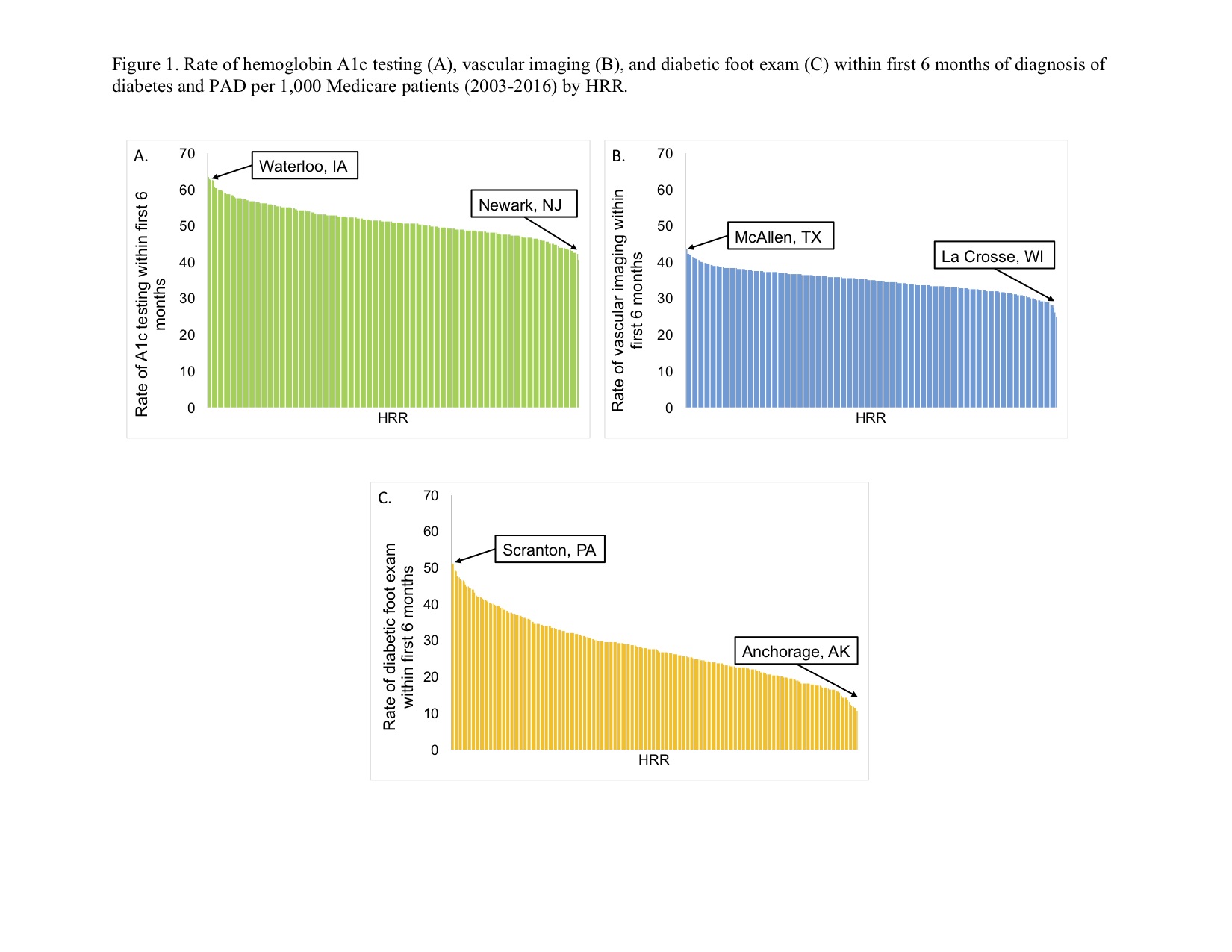
Back to 2020 ePosters