
Endovascular Abdominal Aortic Aneurysm Repair In Octogenarians Is Associated With Higher Risk Of Mortality Compared To Non-octogenarian Geriatric Patients
William Q. Duong, MD, Areg Grigorian, MD, Jeffry Nahmias, MD MHPE, Nii-Kabu Kabutey, MD, Cyrus Farzaneh, MD, Carlos Donayre, MD, Isabella Kuo, MD, Anthony Chau, MD, Roy Fujitani, MD.
University of California, Irvine, Orange, CA, USA.
OBJECTIVES: Geriatric patients (GPs) constitute a growing portion of the general population, with particular increase in the prevalence of octogenarians. The incidence and prevalence of abdominal aortic aneurysms (AAA) have been clearly shown to be associated with advancing age. The effect of advanced age in outcomes from endovascular aortic repair (EVAR) is unclear. We study the effect of advanced age, as an independent risk factor for mortality in octogenarians compared to non-octogenarian GPs undergoing EVAR.
METHODS: The 2011-2017 American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) Procedure-Targeted Vascular database was queried for GPs (>65 years) undergoing EVAR for symptomatic and asymptomatic indications. A multivariable logistic regression analysis was performed comparing outcomes between octogenarian and non-octogenarian GPs.
RESULTS: Of the 10,490 GPs who underwent EVAR, 7508 (71.6%) were non-octogenarians and 2982 (28.4%) were octogenarians. Octogenarians were less often male (76.7% vs. 82.3%). In comparison to non-octogenarian GPs, fewer octogenarian GPs were treated for AAA <5.5 cm (46.7% vs. 54.9%, p<.001) and AAA < 5.0 cm (19.2% vs. 24.0%, p<0.001). Octogenarians had a less dyspnea (15.3% vs. 17.3%, p=0.01), chronic obstructive pulmonary disease (16.1% vs. 20.5%, p<0.001), diabetes (12.7% vs. 17.8%, p<0.001), and smoking (13.2% vs. 36.3%, p<0.001) compared to non-octogenarians. Octogenarians were found to have a greater length of stay (2 days vs. 1 day, p<0.001), as well as rate of mortality (3.4% vs. 1.7%, p<0.001). Multivariate logistic regression analysis showed octogenarians to have increased overall risk of mortality compared to non-octogenarian GP (OR 1.88, CI 1.39-2.54, p<0.001) (Table 1).
CONCLUSIONS: Octogenarians accounted for over a quarter of GPs undergoing EVAR. This elderly group was associated with an increased rate and risk of mortality compared to non-octogenarian GPs, even when controlling for known risk factors for mortality. Given this increased risk of mortality in octogenarians undergoing EVAR, elective treatment of AAAs in this advanced age group should be performed with caution, particularly in those with diameters in which the risk of rupture may not warrant repair. 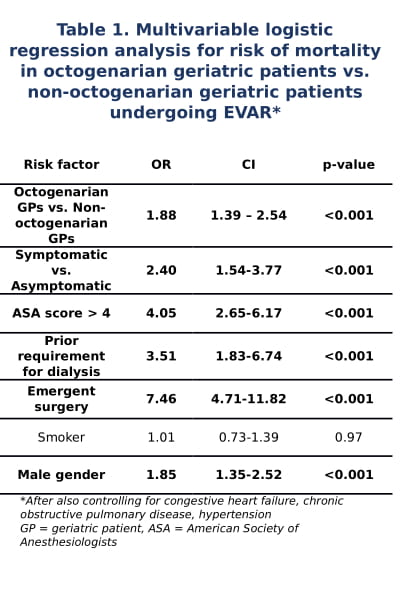
Back to 2020 ePosters