
Utilization And Outcomes Of Regional Anesthesia For Carotid Endarterectomy
Shunella Lumas1, Walter Hsiang1, Shamsuddin Akhtar, MD2, Cassius Iyad Ochoa Chaar, MD3.
1Yale University School of Medicine, New Haven, CT, USA, 2Yale Department of Anesthesiology, New Haven, CT, USA, 3Yale Department of Surgery, Division of Vascular Surgery, New Haven, CT, USA.
OBJECTIVES: The choice of anesthetic for carotid endarterectomy (CEA) continues to be controversial. Recent literature suggests improved outcomes with the use of regional anesthesia (RA) compared to general (GA). The objective of this study is to examine the utilization and outcomes of RA for CEA using a national database.
METHODS: The targeted CEA files of the ACS-NSQIP (2011-2017) were reviewed. Patients were stratified based on anesthesia type into RA and GA, and patients’ characteristics were compared between the 2 groups. The outcomes of CEA under GA and RA were compared after 2:1 propensity matching.
RESULTS: There were 26,206 CEAs, and 14% (n=3,664) were performed under RA, with no change in relative utilization during the study period (p=0.557). Patients treated under RA were more likely to be older than 65 (80.6% vs. 75.8%, p<0.001) and white (90.8% vs. 83.5%, p<0.001), but less likely to have diabetes (28.2% vs. 31.2%, p=0.001), COPD (10.2% vs. 10.5%, p<0.001), heart failure (1.0% vs. 1.5%, p=0.02), and be symptomatic (37.4% vs. 42.7%, p<0.001). After matching, there was no significant difference in baseline characteristics between the 2 groups. Patients undergoing RA were less likely to experience the combined endpoint of stroke, myocardial infarction, or mortality compared to GA. GA patients were more likely to have longer operating time and hospital length of stay (see table).
CONCLUSIONS: CEA performed under RA is associated with improved outcomes compared to GA. RA is underutilized in carotid surgery and strategies to optimize its use are needed. 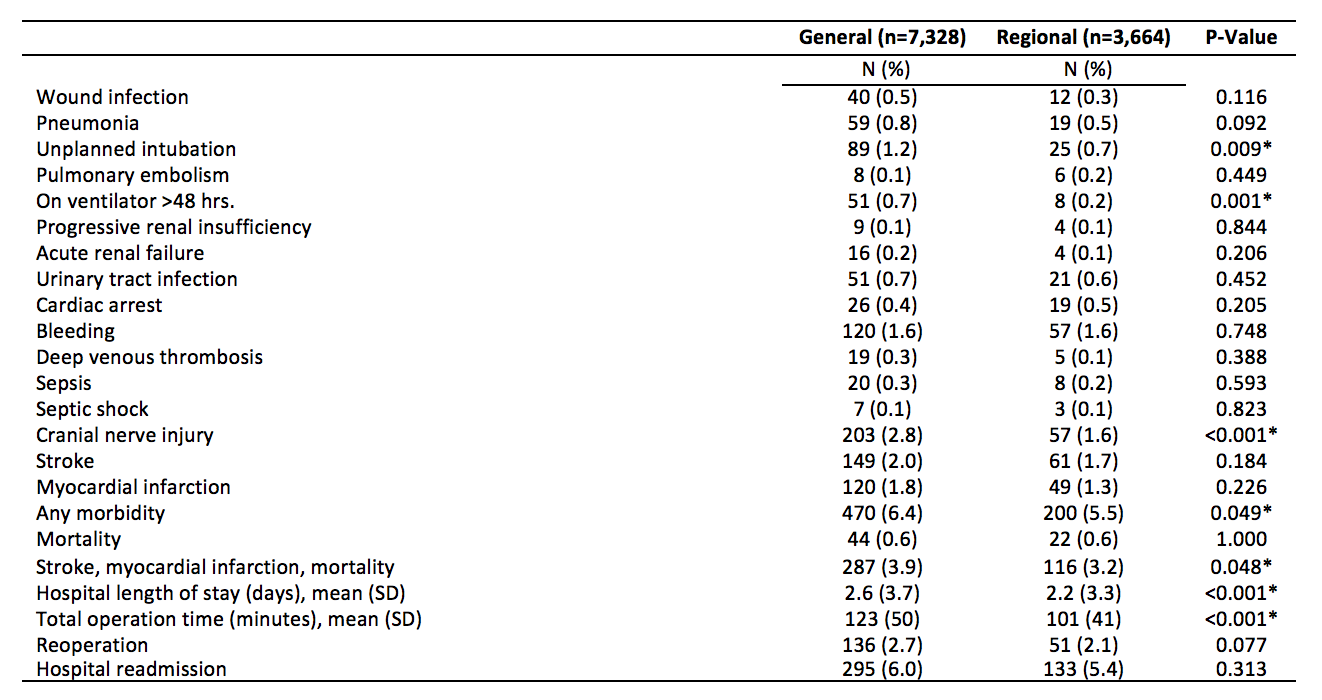
Back to 2020 ePosters