
Retrograde Endovascular With Intimal Re-entry Through Endarterectomy: The REWIRE Technique
Jordan R. Stern, M.D.1, Patrick C. Thompson, MD1, Peter H. Connolly, MD2, Andrew J. Meltzer, MD3.
1Stanford University, Stanford, CA, USA, 2Weill Cornell Medicine, New York, CA, USA, 3Mayo Clinic Arizona, Phoenix, AZ, USA.
OBJECTIVES: Hybrid lower extremity revascularization consisting of common femoral endarterectomy (CFE) and concomitant endovascular intervention has been well described. The typical approach consists of CFE followed by direct patch puncture and treatment. Here, we describe a modified technique that obviates the need for endovascular re-entry and simplifies treatment at the proximal and distal endpoints.
METHODS: The REWIRE technique begins with retrograde arterial access via a patent pedal, tibial, or femoropopliteal vessel (A). The diseased segment is crossed in a retrograde fashion in the subintimal plane. Once the wire reaches the common femoral artery (B), the vessel is surgically exposed. Arteriotomy is performed and the wire is externalized during standard CFE (C). With through-wire access across the diseased segment, a sheath is inserted (D) and the distal disease is treated (E). The proximal extent of the endovascular revascularization is incorporated into a standard CFE with patch angioplasty.
RESULTS: 4 patients (3 male) with chronic limb-threatening ischemia (Rutherford 5) have been treated with this approach. All patients had long segment, chronic total occlusions of the SFA with significant common femoral artery disease. Retrograde access sites included the posterior tibial (1), popliteal (1), distal SFA (1), and occluded SFA stent distal to a fracture site (1). In 3 patients, the distal disease was treated with covered stent placement. Bovine pericardial patch was used for CFE in all. Technical success was achieved in all patients. There were no complications related to the retrograde puncture site, which was controlled with manual pressure (1) or excluded with a covered stent (3). 30-Day freedom from major adverse limb events was 100%. One patient died of myocardial infarction 10 days post-operatively; amputation-free survival is 75% through a mean follow-up of 297 days (range 10-1095) and limb salvage is 100%.
CONCLUSIONS: The REWIRE technique is an effective approach to hybrid revascularization involving the common femoral artery. By traversing the occluded segment in a retrograde fashion and externalizing the wire during CFE, the proximal and distal endpoints can be addressed with relative ease. This obviates the need for endovascular re-entry, and the profunda femoris can be protected under direct visualization. 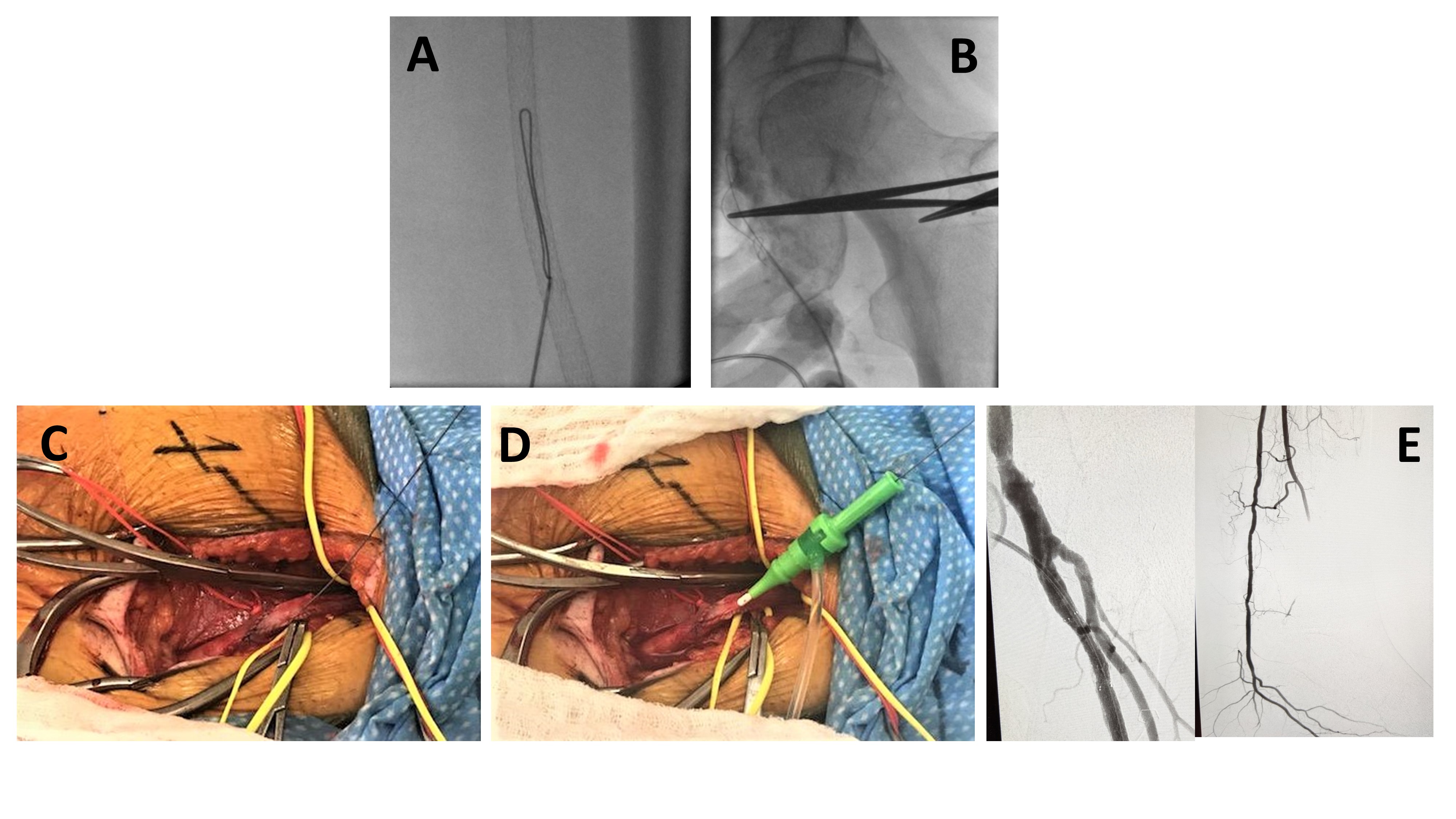
Back to 2020 ePosters