
Females Undertreated For Vascular Disease By Vascular Quality Initiative Analysis
Katharine L. McGinigle1, Sydney E. Browder, BS1, Sherene Shalhub, MD MPH2, Linda M. Harris, MD3, Samantha D. Minc, MD MPH4.
1University of North Carolina, Chapel Hill, NC, USA, 2University of Washington, Seattle, WA, USA, 3University of Buffalo, Buffalo, NY, USA, 4West Virginia University, Morgantown, WV, USA.
Objective:
The first annual Women's Vascular Summit highlighted the knowledge gaps in how females present with vascular diseases and how interventions and outcomes may be impacted by sex. In general, compared to males, females tend to have atypical symptoms and present later, which makes accurate prevalence measurements difficult. We aim to compare the proportion of operations performed for abdominal aortic aneurysms (AAA), cerebrovascular disease (CVD), and peripheral arterial disease (PAD) by sex.
Methods:
Prevalence of AAA, CVD, and PAD was obtained from the National Institute of Health and the Agency for Healthcare Research and Quality data. Procedural data for 6 vascular operations were obtained from the Vascular Quality Initiative (VQI) for the period of 2014-2019: open AAA repair, endovascular AAA repair (EVAR), carotid endarterectomy and stenting, infrainguinal bypass, and endovascular peripheral arterial intervention. The proportion of females and males undergoing each operation were compared using student t-tests. Age, race, and comorbidities were compared using chi-square tests. Finally, the expected treatment rates were calculated from prevalence data, and compared to actual treatment rates.
Results:
Over the last 5 years, a total of 345,873 procedures were performed with females accounting for 36% of all procedures. There were no differences in comorbidities between sexes; however, females were slightly older than males (mean age 69.9 ± 11.2 vs. 69.1 ± 10.3 years, P<0.001) at the time of the procedure. Females were significantly less likely to undergo any of these 6 procedures compared to males
(P<0.001). Based on estimated disease prevalence, females undergo fewer interventions for AAA, carotid stenosis, and PAD than expected compared to males (Table 1).
Conclusions:
Females do not get treated for AAA, carotid stenosis, and, especially, PAD at the expected rate based on disease prevalence. A broader understanding of current vascular practices and sex-specific disease presentation and management are required to explore ways of addressing the sex-disparity in vascular disease care. 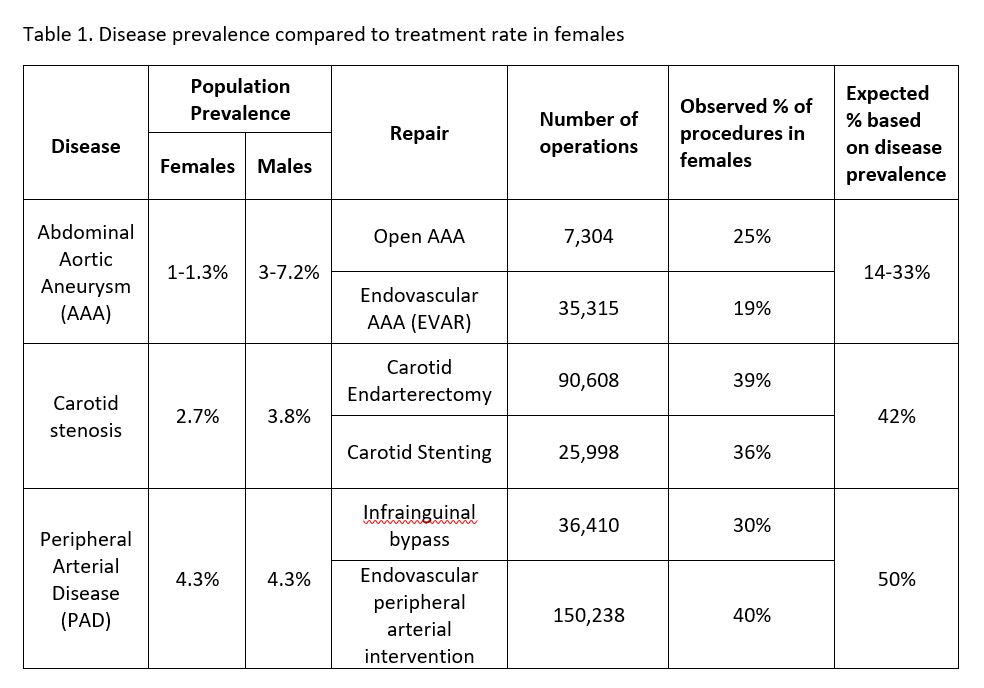
Back to 2020 ePosters