
Non-Hispanic Black And Hispanic Patients Experience Inferior Limb Outcomes But Equivalent Or Improved Cardiovascular Outcomes In Comparison To White Patients After Infrainguinal Revascularization
Corey A. Kalbaugh, PhD1, Alexander Shannon, MD2, Brian Witrick, MPH1, Katharine L. McGinigle, MD3, Bryan A. Ehlert, MD4, William P. Robinson, MD5.
1Clemson University, Clemson, SC, USA, 2University of Virginia, Charlottesville, VA, USA, 3University of North Carolina at Chapel Hill, Chapel Hill, NC, USA, 4East Carolina University, Greenville, SC, USA, 5East Carolina University, Greenville, NC, USA.
Objective. The purpose of this study was to compare limb and cardiovascular outcomes among racial/ethnic groups after infrainguinal revascularization and to investigate whether differences in preoperative care account for disparities.
Methods. The Vascular Quality Initiative infrainguinal bypass and peripheral vascular intervention (PVI) modules were queried to identify patients undergoing revascularization between 2011 and 2018. Procedures for acute limb ischemia, suprainguinal disease, and emergent cases were excluded. The primary exposure variable was race/ethnicity, including non-Hispanic White (White; referent), non-Hispanic Black (Black), and Hispanic. Patients of other races/ethnicities were excluded. Primary outcomes were in-hospital major adverse limb events (MALE; defined as major amputation or reintervention), major amputation, major adverse cardiac events (MACE; defined as myocardial infarction, stroke, or death), and survival. Multivariable regression was used to identify factors independently associated with in-hospital outcomes.
Results. Among 118,944 revascularizations, 90,798(76%) were performed in White, 20,808(18%) in Black, and 7,338(6%) in Hispanic patients. A higher proportion of Black and Hispanic patients presented with critical limb ischemia and were on dialysis (ESRD) compared to Whites. White patients were more likely to be current smokers and to have COPD compared to Black and Hispanic patients. Pre-procedure aspirin use was statistically lower among Blacks and Hispanics compared to Whites. Pre-procedure statin use was lower in Blacks compared to Hispanics and Whites. Medication differences were not clinically remarkable. MALE and major amputation were significantly higher in Blacks and Hispanics as compared to Whites (Table). In adjusted analyses, Blacks were 1.4 and 1.8 times as likely as Whites to experience MALE and major amputation, respectively. Hispanic patients were 1.5 and 2.0 times as likely as Whites to experience MALE and major amputation, respectively. MACE were less common among Blacks compared to Whites and equivalent between Hispanic and White patients. There were no survival differences between groups.
Conclusions. Blacks and Hispanics experienced early adverse limb outcomes nearly twice as frequently as White patients. Blacks experienced cardiovascular morbidity less commonly and mortality did not differ between racial/ethnic groups. Medication usage did not explain the marked difference in limb outcomes. Improved approaches to treating Black and Hispanic patients with infrainguinal PAD are needed. 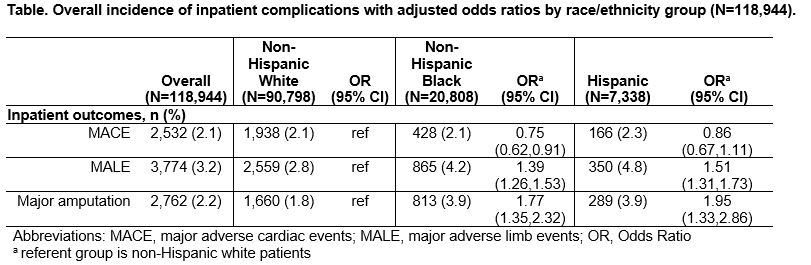
Back to 2020 ePosters