
Rapid, Midline Retroperitoneal Exposure For 4-level Anterior Lumbar Interbody Fusion
Rema Malik
Wayne State University, Detroit, MI
DEMOGRAPHICS: A 77-year old female presents with decades of worsening, now intractable back pain related to kyphosis with significant compression of her cartilaginous disc spaces throughout her lumbar spine.
HISTORY: We describe a novel, rapid midline retroperitoneal operative technique who underwent an extensive L2-S1 anterior lumbar interbody fusion in addition to posterior instrumentation.
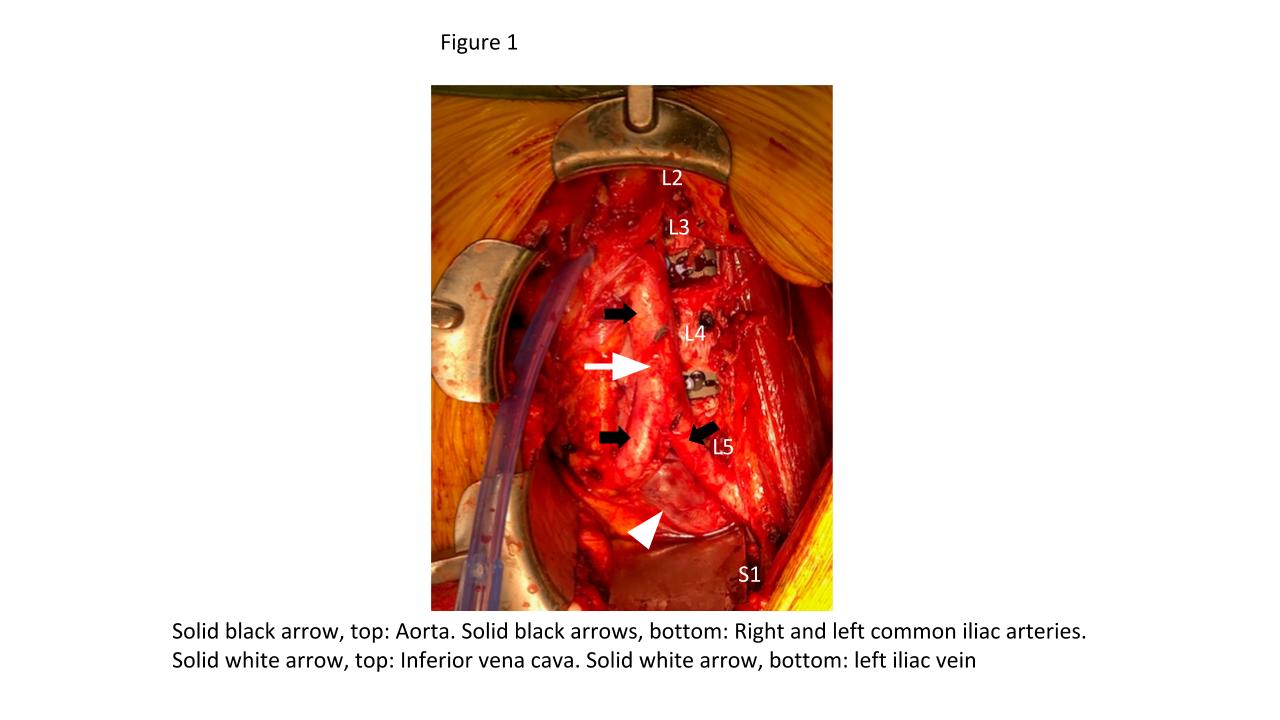
PLAN: A longitudinal incision was fashioned between the L3-S1 segments, with skin and subcutaneous tissues dissected down to the linea alba, subcutaneous tissues cleared to the left of midline, and anterior rectus sheath incised. We exposed only the medial rectus abdominis muscle, dissecting this portion off the posterior rectus sheath, and bluntly exposing the posterior rectus sheath with gentle upward exposure of the posterior rectus sheath, visualizing the arcuate line, with transversalis fascia immediately seen inferiorly. The peritoneum was mobilized and a bookwalter retractor placed. Due to her high riding pelvic brim, the IVC confluence and aortic bifurcation overlaid the L5-S1 segments. The iliolumbar vein and surrounding lumbar vessels from the aorta and inferior vena cava were carefully dissected and ligated in order to mobilize the patient's left iliac vein towards the right side during exposure of the L5-S1 segment. Small lumbar vessels and the middle sacral vessels were clipped. The abdominal aorta and iliac veins were retracted toward the patient's right side. Exposure to the L2 level was facilitated by mobilization of the retroperitoneum and clipping remaining lumbar vessels to allow handheld retraction of the aorta and IVC toward the right side.
DISCUSSION: The commonly used left lower abdominal transverse and paramedian incisions require significant mobilization of the left rectus muscle with increased abdominal wall morbidity, likelihood for rectus sheath hematoma and suboptimal retraction of spine centering during intraoperative radiography. Our approach enables an essentially midline approach to the rectus muscle and uses the diminution of the transversalis fascia-to-peritoneum transition in the pelvis to provide expedited exposure for L5-S1, L4-L5 exposures, and multilevel exposures.
Back to 2021 Abstracts