
74 Year Old Man With Occluded Axillo-bi-femoral Bypass, Hostile Abdomen, And Multiple Groin Incisions
Nolan C. Cirillo-Penn, MD, Manju Kalra, MBBS
Mayo Clinic, Rochester, MN
Demographics: 74 year-old man presenting with worsening bilateral lower extremity sub-acute ischemia.
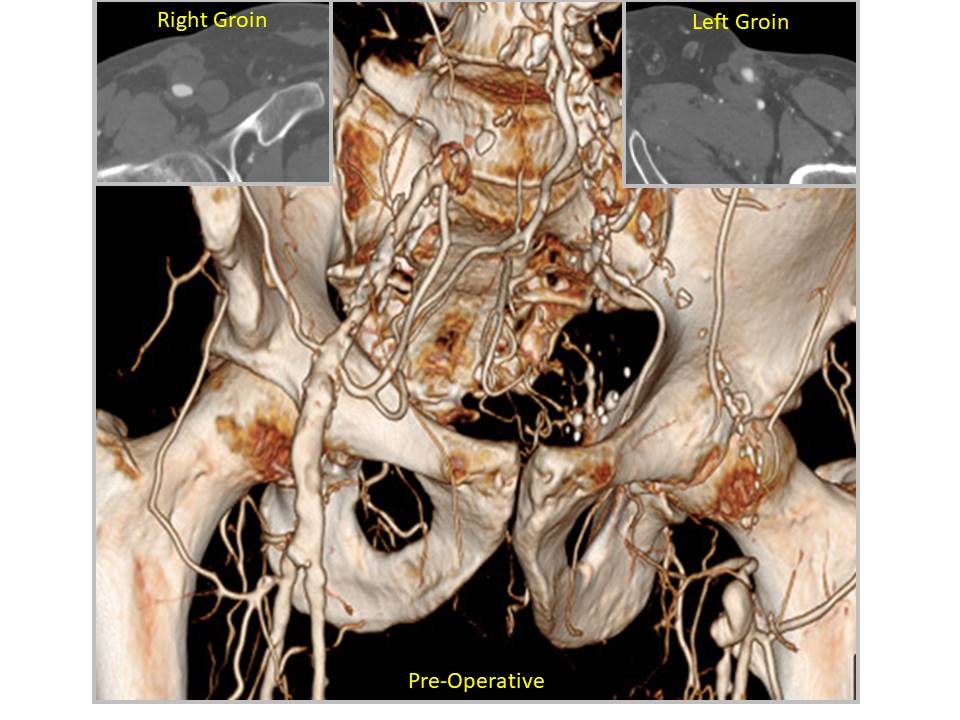
HISTORY: The patient presented with several month history of progressive claudication, gait instability and cool feet, left lower extremity (LLE) worse than right and was found on CTA to have occlusion of his left axillo-bi-femoral bypass (ABFG) and aneurysmal femoral anastomoses (Figure 1). The ABFG along with LLE thrombectomy and fasciotomy was performed 5 years previously following acute occlusion of an aorto-bi-iliac graft for 8 cm AAA repair placed 4 years before. He had suffered multiple complications of the ABFG in the form of groin wound infection and pseudoaneurysms treated with eventual sartorius muscle flap cover after complete replacement of the crossover limb with cryopreserved vein and eventually partial replacement of this and parts of the main limb with cryopreserved arterial conduit over the next 2 years. One year previously open thrombectomy was performed for graft occlusion following endovascular intervention for stenosis.
PLAN: The multiple time re-do groin interventions with existing muscle flaps, hostile abdomen, possible residual infection, and cryopreserved vein allograft with aneurysmal degeneration posed significant challenges. Re-do aortic reconstruction was planned after ruling out residual infection with a PET/ CT scan. Bilateral groins were dissected again to expose the femoral vessels and the sartorius flaps were preserved. Left posterolateral thoracotomy was performed through the 7th intercostal space and a Rifampin soaked, ringed 10 mm dacron graft was anastomosed end-to-side to the partially clamped descending thoracic aorta. The graft was tunneled through the posterior diaphragm and left retroperitoneal space to the left groin, facilitated with a short flank incision. A crossover femoro-femoral limb of Rifampin soaked 8 mm dacron graft was attached. All prior cryopreserved material in both groins was excised and femoral reconstructions were performed, including an interposition right femoral graft. The Sartorius flaps were replaced and the groins closed. His postoperative course was uncomplicated with dismissal home on day 10. LLE ankle brachial indices improved from 0.28 to 0.87.DISCUSSIONThoraco-bi-femoral bypass is an excellent option in patients with multiple prior failed aortic reconstructions.
Back to 2021 Abstracts