
Outcomes of Transcarotid Artery Revascularization and Carotid Endarterectomy at a Single Institution
Christopher Cappellini, DO, MS1, Hong Zheng, DO2, Kathleen M. Lamb, MD2, Renganaden Sooppan, MD2, Robert Q. Luo, DO2.
1Philadelphia College of Osteopathic Medicine, Philadelphia, PA, USA, 2Reading Hospital, Tower Health, Reading, PA, USA.
OBJECTIVES:Carotid endarterectomy (CEA) and carotid artery stenting (CAS) are accepted revascularization modalities to treat carotid artery disease. Higher incidences of perioperative adverse neurological events and death have been reported in transfemoral CAS patients. Transcarotid artery revascularization (TCAR) is a newer operative technique that involves direct transcervical carotid access, mitigating aortic arch manipulation and minimizing the risk of embolic stroke via cerebral blood flow reversal. Perioperative stroke, myocardial infarction (MI), and death rates have been shown to be similar between TCAR and CEA, with TCAR having less complications. The objective of this study was to ascertain the safety and viability of TCAR in a community hospital setting by evaluating perioperative outcomes. We hypothesized that patients undergoing TCAR and CEA have equivalent outcomes.
METHODS:We performed a single institution retrospective review of a prospectively maintained Vascular Quality Initiative database on patients who underwent TCAR or CEA between 2012 and 2019. A total of 66 TCAR cases from February 2018 to December 2019 and 501 CEA cases from January 2012 to December 2019 were reviewed. Preoperative, intraoperative, and postoperative characteristics as well as perioperative outcomes were captured for the statistical analyses.
RESULTS:From 2012 to 2019, 567 patients underwent TCAR or CEA. TCAR patents were found to have higher rates of comorbidities compared to CEA, including CAD and CHF. There were zero procedure-related strokes in patients that underwent TCAR compared to five in CEA patients (0% vs 1.0%, P = 0.42). The CEA procedure-related strokes were due to technical problems resulting in stenosis or thrombosis of the target vessels. Overall, there were no perioperative deaths, MI, cranial nerve injury (CNI), or hematoma in patients who underwent TCAR. There were no complications of thrombosis, surgical site infection, pseudoaneurysm, or arteriovenous fistula among TCAR or CEA patients.
CONCLUSIONS:This single-center retrospective analysis of TCAR and CEA for the treatment of carotid artery disease suggests TCAR can result in less perioperative procedure-related stroke compared to CEA as well as less perioperative complications including MI, CNI, hematoma, and death. Therefore, TCAR may be considered a safe, feasible carotid revascularization option even in a community hospital setting. 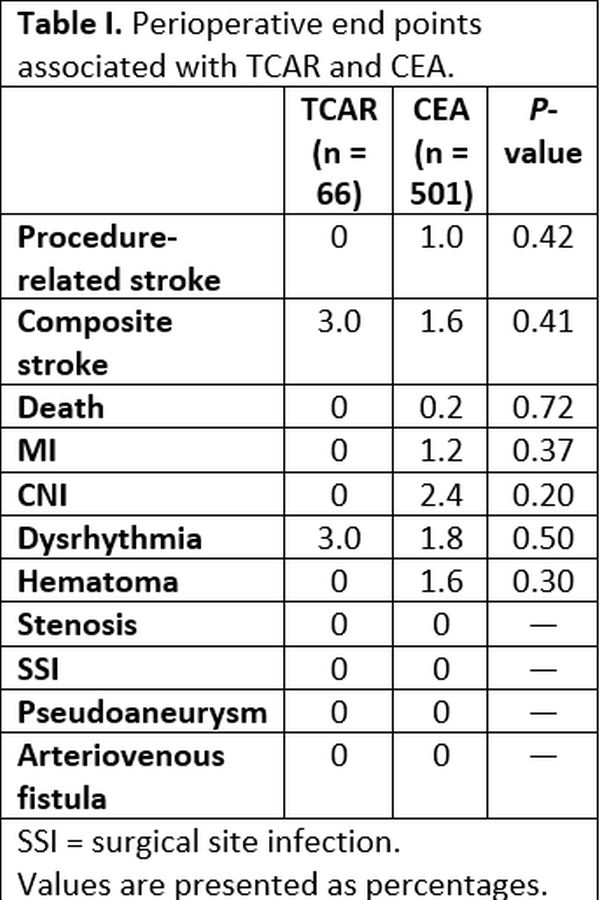
Back to 2021 Karmody Posters