
Risk Analysis Index: What Can It Tell Us About Veterans Undergoing Lower Extremity Bypass
Sally Boyd, MD, Kedar S. Lavingia, MD, Wayne Tse, MD, Michael F. Amendola, MD, MEHP.
Virginia Commonwealth University, Richmond, VA, USA.
OBJECTIVES: Studies have shown an association between preoperative frailty and poor postoperative outcomes following lower extremity bypass (LEB) procedures. The Risk Analysis Index (RAI) is a validated measure of frailty that has been used to predict clinical outcomes. We applied the RAI measure to patients having undergone LEB in a veteran population and assessed procedural morbidity and mortality as it relates to preoperative frailty.
METHODS: The Veteran’s Affairs Surgical Quality Improvement Program (VASQIP) database was assessed for patients who underwent LEB. Variables examined included complications, return to the operating room, graft failure, and death. Only femoral to distal bypasses were included in the analysis. RAI was calculated using the recalibrated RAI-A and patients fell into three separate cohorts: non-frail (RAI< 30), frail (RAI 30-34), and very frail (35 or higher). Chi squared* and ANOVA† were used to assess the differences between these groups.
RESULTS: From 1998 to 2018, 79,521 patients underwent lower extremity bypass. The average age was 64.2 years old and 99% patients were male. Preoperative frailty was associated with higher rates of graft failure with odds ratios 1.225 (95% CI 1.114-1.347) in frail and 1.366 (95% CI 1.235 - 1.511) in very frail patients. Additionally, patients in the higher-scoring RAI groups had longer hospital stays. 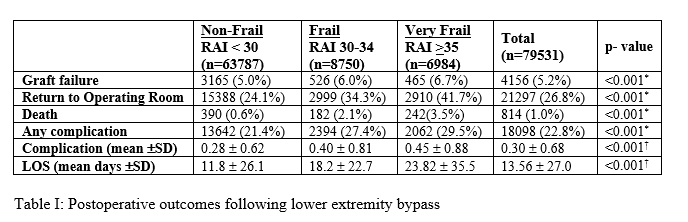 They also were more likely to return to the operating room, OR 1.640 (95% CI 1.564-1.720) for frail patients and 2.247 (95% CI 2.135-2.364) for very frail patients. They experienced a higher complication rate with OR 1.384 (95% CI 1.316-1.456) for frail and 1.540 (95% CI 1.458 - 1.627) for very frail. They were at higher risk of death OR 3.452 (95% CI 2.892-4.123) for frail and 5.835 (95% CI 4.961-6.863) for very frail.
They also were more likely to return to the operating room, OR 1.640 (95% CI 1.564-1.720) for frail patients and 2.247 (95% CI 2.135-2.364) for very frail patients. They experienced a higher complication rate with OR 1.384 (95% CI 1.316-1.456) for frail and 1.540 (95% CI 1.458 - 1.627) for very frail. They were at higher risk of death OR 3.452 (95% CI 2.892-4.123) for frail and 5.835 (95% CI 4.961-6.863) for very frail. 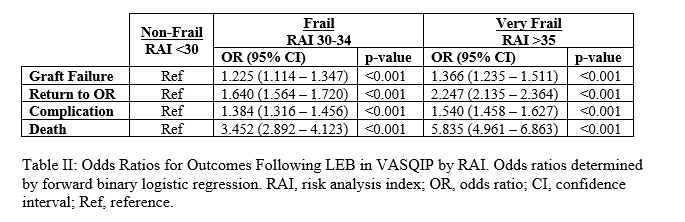
CONCLUSIONS: Preoperative frailty as measured by the RAI was significantly associated with postoperative complications, graft failure, return to the operating room, longer hospital stays, and death. Careful consideration should be given to both patient selection and preoperative optimization in patients undergoing LEB.
Back to 2021 ePosters