
Postoperative Outcomes In Patients With Hostile Neck Anatomy Undergoing Transcarotid Artery Revascularization
Maryam A. Khan, MD, Nadin Elsayed, MD, Rohini J. Patel, MD, MPH, Jonathan Unkart, MD, MPH, Louis Cajas-Monson, MD, Mahmoud B. Malas, MD, MHS.
University of California San Diego, San Diego, CA, USA.
OBJECTIVES: With hostile neck anatomy being a relative contraindication to Carotid Endarterectomy (CEA), Carotid Artery Stenting (CAS) is frequently employed for carotid revascularization among these patients. However, this could potentially increase the risk of periprocedural complications. As Transcarotid Artery Revascularization (TCAR) has progressively replaced CAS in the past few years, evidence pertaining hostile neck anatomy and TCAR is necessary to establish its safety and feasibility in this subgroup of patients. Therefore, we aimed to analyze the impact of hostile neck anatomy on outcomes in patients undergoing TCAR.
METHODS: All patients undergoing TCAR from November 2016-June 2021 in the Vascular Quality Initiative (VQI) Database were included. Patients were characterized into the two groups based on the neck anatomy. Hostile neck anatomy was defined as history of neck irradiation or prior neck surgery including prior CEA or radical neck dissection. Outcomes included technical failure, access site complications (hematoma, stenosis, infection, pseudoaneurysm and AV fistula), stroke, TIA, MI, death, and composite endpoints of stroke/death, and stroke/TIA. Univariable and multivariable logistic regression was used to assess impact of hostile neck anatomy on postoperative outcomes and results were adjusted for relevant potential confounders.
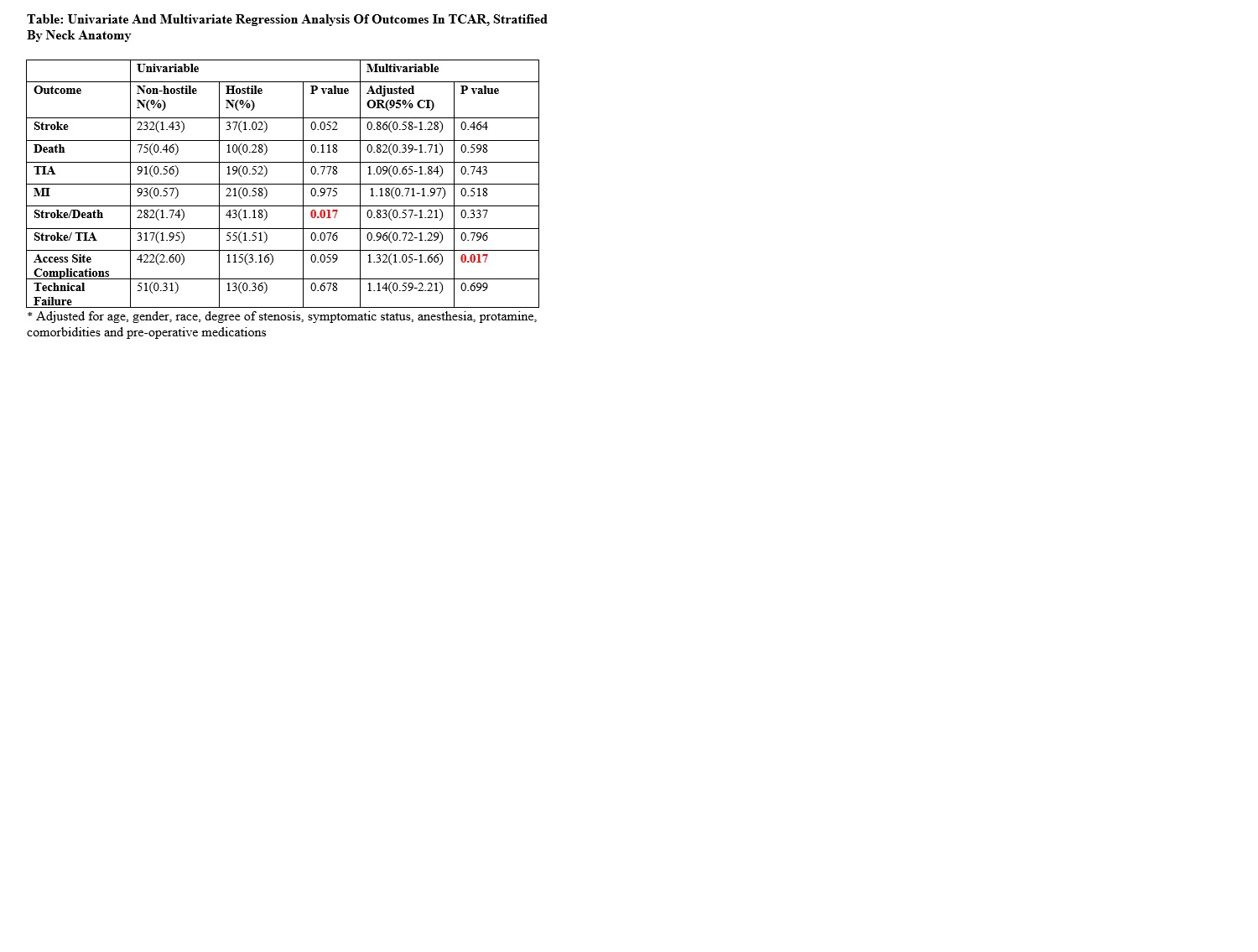
RESULTS: Of the total 19,859 who underwent TCAR during the study period, 3636(18.3%) had hostile neck anatomy while 16223(81.7%) had non-hostile neck anatomy. Patients with underlying hostile neck were more likely to be younger (70.9 vs 73.9, p<0.001), have fewer comorbidities, but were more likely to be active smokers(23.8% vs 21.2%, p<0.001), and have high degree of stenosis(56.0% vs 49.0, p<0.001). On univariate analysis, both groups had comparable outcomes except for higher rates of stroke/death in patients with hostile neck anatomy. After adjusting for potential confounders, there were no differences in technical failure, stroke, death and MI. However, patients with hostile neck were at 32% increased risk of access site complications(aOR: 1.32(1.05-1.66, p=0.017).(Table)
CONCLUSIONS: Patients with hostile neck anatomy experienced an increased risk of access site complications, however, the risk for technical failure and postoperative Stroke, TIA, MI, or death was similar in both groups. These results confirm that TCAR can be safely utilized in patients with hostile neck anatomy for carotid revascularization.
Back to 2022 Karmody Posters