
The Impact Of Large-Bore Access Complications On Outcomes Of Patients Undergoing TEVAR
Abhishek Devaguptapu Rao, BA/BS1, Priya B. Patel, MD MPH2, Ambar Mehta, MD MPH1, Danielle Bajakian, MD1, Nicholas Morrissey, MD1, James Iannuzzi, MD MPH3, Karan Garg, MD4, Marc Schermerhorn, MD5, Jeffrey J. Siracuse, MD MBA6, Hiroo Takayama, MD PhD1, Virendra I. Patel, MD MPH1.
1Division of Cardiac, Thoracic, and Vascular Surgery, NYP-Columbia University Medical Center, New York, NY, USA, 2Division of General Surgery, Rutgers-Robert Wood Johnson Medical School, Brunswick, NJ, USA, 3Division of Vascular Surgery, U California San Francisco School of Medicine, San Francisco, CA, USA, 4Division of Vascular and Endovascular Surgery, NYU School of Medicine, New York, NY, USA, 5Division of Vascular and Endovascular Surgery, Beth Israel Deaconess Medical Center, Boston, MA, USA, 6Division of Vascular and Endovascular Surgery, Boston University, Boston, MA, USA.
Objective:
TEVAR is increasingly used to treat aortic dissection and aneurysms. Access-related complications remain a common source of morbidity and mortality following TEVAR. Therefore, this study aims to determine major risk factors predicting access complications in patients and five-year survival in patients with access complications.
Methods:
We identified all patients undergoing TEVAR in the VQI from July 2010 to April 2020, excluding those converted to open operation. We defined access complication as post-operative occlusion, wound infection, hematoma, or unplanned conversion to open cutdown. The primary outcome was 5-year-survival and the secondary outcome was perioperative mortality. Mixed-effects logistic regression modelling with physician level clustering was used to identify factors associated with access complications and perioperative mortality. Kaplan-Meier estimates and Cox-Proportional Hazards Models were used for analysis of five-year survival.
Results:
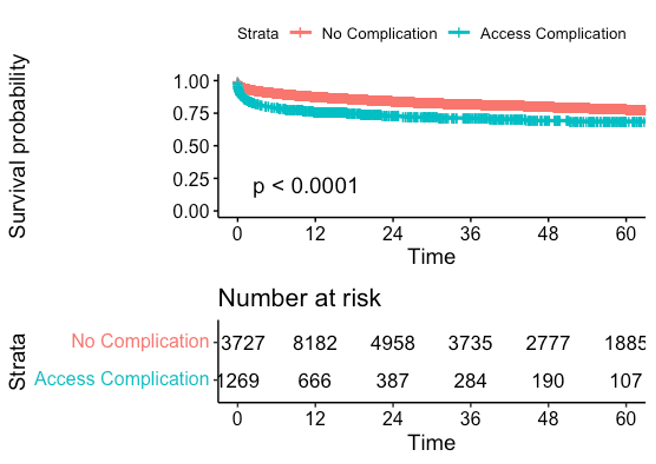
Of 14,997 patients, 1269 (8.5%) had access complications. Bilateral percutaneous access was obtained in 66% of patients, one percutaneous and one open in 15% and bilateral open access in 15%. Patients with access complications were older (70±12.9 vs. 67 ±14.6, p<.01) and female (51% vs. 34%, P <.01). Patients with access complications experienced increased perioperative mortality (12% vs. 5.0%, p<.01), MACE (17% vs 7.5%, P<.01), reintervention (24% vs. 10% , P<.01), and spinal ischemia (7.5% vs. 2.6%, P<.01). On adjusted analysis, factors associated with access complication include female sex (OR:2.2 [1.7-2.8]; P<.01), BMI (OR:0.86 [0.78-0.95]; p<.01), Hispanic ethnicity (OR:1.8 [1.0-3.1], p<.05). Access complication was independently associated with perioperative mortality (OR:2.1, [1.6-2.9], p<.01). Bilateral cutdown was associated with decreased mortality in men (OR:0.39, [0.23-0.67], p<.01) but not women (OR:2.9, [1.4-6.2], p<.01). Lastly, access complications were associated with increased five-year mortality (HR:1.4, [1.1-1.7], p<.01).
Conclusions:
Access complications when unexpected are associated with adverse perioperative and five-year outcomes. Female sex is associated with increased rates of access complications, suggesting the need for devices tailored to female anatomy.
Back to 2022 Karmody Posters