
Medical Center Reimbursement For Vascular Procedures Has Increased Over Time While Professional Reimbursement Has Declined
Zachary B. Fang, MD, MSc1, Andres Schanzer, MD1, Dejah R. Judelson, MD1, Douglas R. Jones, MD1, Jessica P. Simons, MD, MPH1, William Sheaffer, MD2, Andrew J. Meltzer, MD, MBA2, Francesco A. Aiello, MD, MBA1.
1University of Massachusetts Medical School, Worcester, MA, USA, 2Mayo Clinic Arizona, Phoenix, AZ, USA.
OBJECTIVES:The US healthcare system uses different methods for assigning medical center reimbursement (MCR) and professional reimbursement (PR) for clinical services. We hypothesize that PR has not increased proportionately to MCR for the same vascular services. METHODS:MCR and PR were compared for commonly performed inpatient and outpatient vascular procedures between 2012 and 2021. MCR was calculated using the Inpatient Prospective Payment System (IPPS) and Outpatient Prospective Payment System (OPPS). PR was calculated using the Medicare Physician Fee Schedule (MPFS). Expected reimbursement was calculated based on observed inflation using consumer price index (CPI). RESULTS:Between 2012-2021, MCR for inpatient procedures increased 20-26% for carotid endarterectomy (CEA), 24-27% for femoral endarterectomy (FEA), 24-27% for femoral-popliteal bypass with vein, 14-19% for thoracic endovascular aortic repair (TEVAR), and 15% for aortobifemoral bypass (AOBF). During the same period, PR increased 3.3% for CEA but decreased for FEA (-5.0%), femoral-popliteal bypass (-4.6%), TEVAR (-4.2%), and AOBF (-5.0%). When comparing expected reimbursement, adjusted for inflation, to actual reimbursement, PR experienced a 10-17% reduction while MCR outpaced inflation by 3.7-10%. For outpatient procedures, MCR increased 117% for tibial angioplasty, 24% for superficial femoral artery (SFA) stenting, 62% for tunneled dialysis catheter (TDC) insertion, and 24% for iliac stenting, but decreased 0.43% for arteriovenous fistula (AVF) creation, and 7.6% for radio frequency ablation (RFA). PR increased 0.91% for SFA stenting but decreased for tibial angioplasty (-17%), AVF creation (-6.4%), TDC insertion (-7.1%), iliac stenting (-3.8%), and RFA (-22%). Comparing expected reimbursement, adjusted for inflation, to actual reimbursement, PR experienced a 13-32% reduction while MCR outpaced inflation 7.5%-88% for tibial angioplasty, SFA stenting, TDC insertion, and iliac stenting, but experienced a reduction for AVF (-13%) and RFA (-19%). CONCLUSIONS:
MCR for commonly performed vascular procedures has increased and outpaced inflation. Conversely, PR for these same services has decreased across all procedure types, especially when adjusted for inflation. This inequity in reimbursement methodology between MCR and PR requires attention as a threat to the viability of the physician workforce. Either changes in reimbursement methodology or reallocation of reimbursement to physicians are imperative to sustain physician practices. 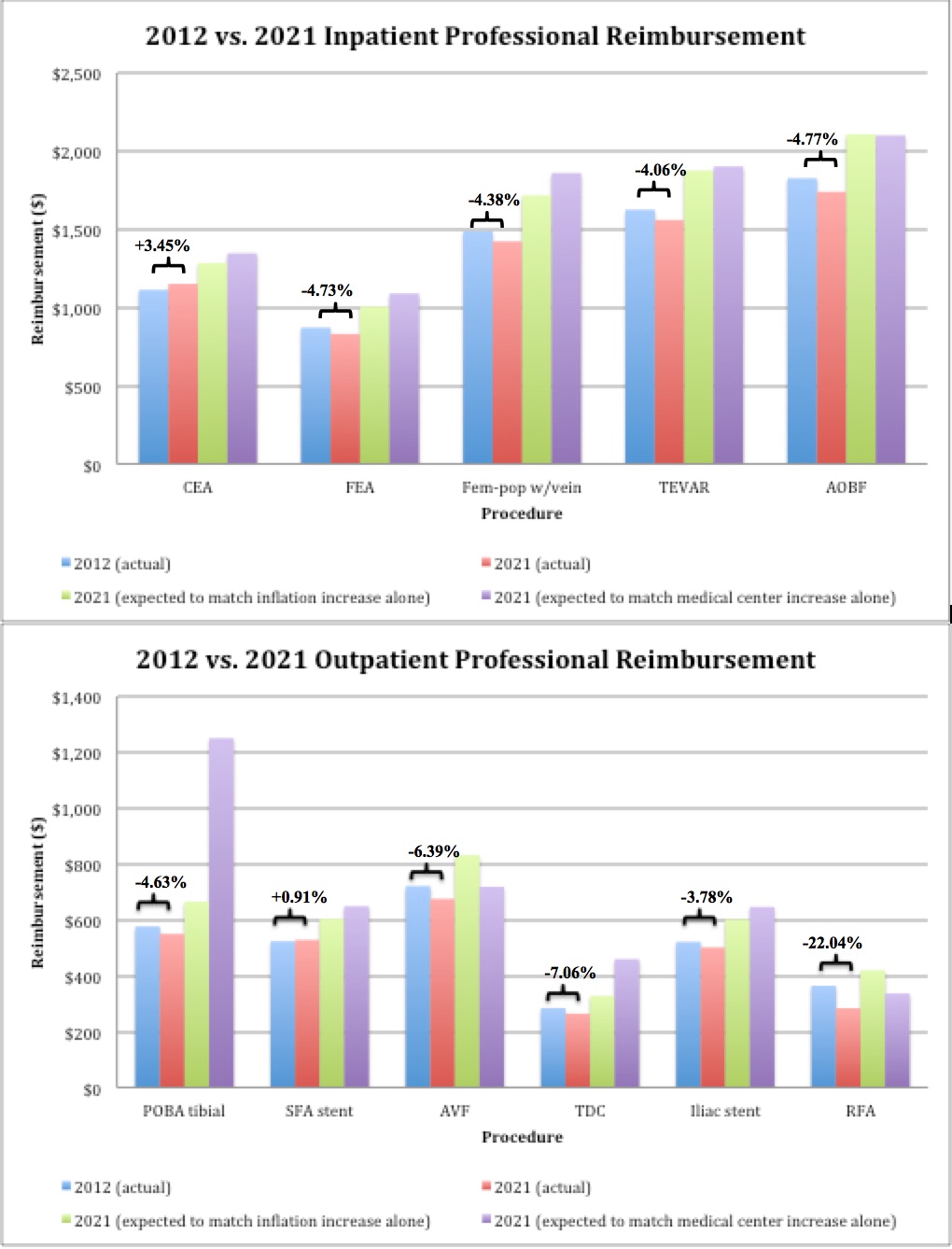
Back to 2022 Abstracts