
Use Of Low-Flow Cardiopulmonary Bypass For Repair Of Complex Abdominal Aortic Aneurysms In Patients With Relative Contraindications To Aortic Cross-Clamping
Nolan C. Cirillo-Penn, MD1, Alberto Pochettino, MD1, Ali H. Khalifeh, MD1, Jill J. Colglazier, MD1, Fahad Shuja, MBBS1, Gustavo S. Oderich, MD2, Thomas C. Bower, MD1.
1Mayo Clinic, Rochester, MN, USA, 2The University of Texas Health Science Center at Houston, Houston, TX, USA.
OBJECTIVES: To evaluate the feasibility of low-flow cardiopulmonary bypass (LFCPB) for repair of complex abdominal aortic pathologies in patients in whom standard repair techniques are not applicable.
METHODS: A single-center, retrospective review of patients undergoing repair of the infrarenal, juxtarenal, and paravisceral aorta with relative contraindications to aortic cross-clamping utilizing LFCPB from 2014-2020 was conducted. This technique was used to minimize atheroembolism, spinal cord, visceral and renal ischemia. Repair was done with a vascular and cardiothoracic surgical team. Demographics and procedural details were reviewed. Endpoints were mortality, morbidity, and freedom from aortic-related mortality.
RESULTS: LFCPB was utilized in 5 patients, which represents well under 1% of total aortic repairs during the time-period. There were 4 males and the mean age was 66±11 years. Aneurysms were degenerative in three and post-dissection in two. Three patients had prior aortic procedures(one Bentall, one EVAR, and one with multiple operations including prior arch, descending thoracic aortic repair, and paravisceral debranching). Another patient had a retrograde ilio-SMA/Celiac bypass with anastomotic pseudoaneurysm. No patient was a candidate for standard open or endovascular repair because of diffuse intraluminal thrombus, complex visceral and renal occlusive disease, and/or an inadequate clamp site. Repair was juxtarenal in three, one of whom needed EVAR explant; paravisceral in one, in which renal and SMA bypasses were necessary; and infrarenal in one to repair aorto-iliac aneurysms below a previous TAAA reconstruction. All patients had axillary artery cannulation with venous cannulation through the femoral vein or at the cavoatrial junction. Mean CPB time was 166 minutes(range: 48-255 minutes). Two patients each needed mild or deep hypothermia. Visceral and renal perfusion cannulas were utilized in two. There were no deaths. Four patients had one or more complications. Acute kidney injury occurred in two(RIFLE class I), but neither required dialysis. Bowel ischemia requiring partial colectomy, chyle leak, pneumonia/respiratory failure, and arrhythmia occurred in one each. No patients had atheroembolization or spinal cord ischemia. At median follow-up of 11 months(range: 3-85) the freedom from aortic-related mortality was 80%.
CONCLUSIONS: LFCPB can be used to repair complex aortic aneurysms in select patients with relative contraindications to aortic cross-clamping. 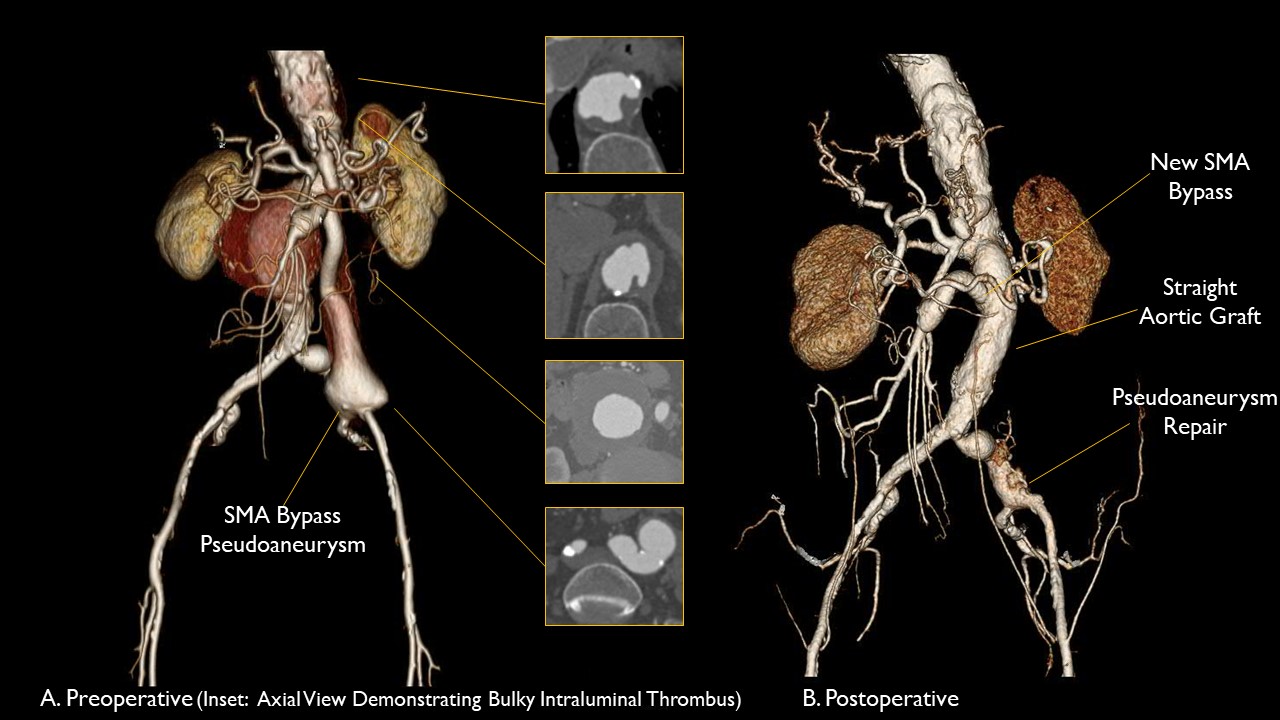
Back to 2022 ePosters