
Identification Of New Patient Groups That Fall Outside Of Currently Established Screening Guidelines For Abdominal Aortic Aneurysm That May Benefit From Screening
Varun K. Dalmia, BA, Matthew Carnevale, MD, Antoine Pham, BA, John Denesopolis, MD, Evan C. Lipsitz, MD, MBA, Jeffrey E. Indes, MD.
Albert Einstein College of Medicine, Bronx, NY, USA.
OBJECTIVES: Previous studies have identified groups of patients with abdominal aortic aneurysm (AAA) that fall outside of currently accepted screening guidelines. Population-based studies have found AAA screening would be cost-effective at a prevalence of 0.5-1%. The goal of this study was to analyze the prevalence of specific groups of patients that fall outside of the current screening guidelines and analyze outcomes of groups with a prevalence of greater than 1%.
METHODS: Using the TriNetX Analytics Network, several patient cohorts were abstracted with a diagnosis of ruptured or unruptured AAA based on previously identified groups with potential high risk for AAA that fall outside of currently accepted screening guidelines. Groups were also stratified by sex. For groups found to have a prevalence of greater than 1% (Table 1), the unruptured patients were further analyzed for long-term rates of rupture and included male ever-smokers 45-65, male never-smokers 65-75, and male never-smokers >75. Long-term mortality was compared with patients without AAA after propensity score matching.
RESULTS: Of patients with intact AAA, male ever-smokers 45-64 had the highest rupture rates of 1.5%, 2.2%, and 2.4% at 1, 5, and 10 years, respectively. Male never-smokers 65-75 had rupture rates of 0.81%, 1.3%, and 1.4% at these time points. Male never-smokers >75 had the lowest rupture rates of 0.78%, 1.2%, 1.3% at these timepoints. Compared to controls, male ever-smokers 45-64 with AAA had greater mortality at 1-year (4.8% vs. 3.6%, p<0.001), 5-years (10.8% vs. 8.5%, p<0.001), and 10-years (13.1% vs. 10.3%, p<0.001). Male-never smokers >75 with AAA also had greater mortality compared with controls at 1, 5, and 10 years (7.3% vs. 4.4%, 16.1% vs. 10.1%, and 18.5% vs. 11.7%, all p<0.001). Similarly, male never-smokers 65-75 with AAA had greater mortality at these timepoints (4.0% vs. 2.6%, 10.3% vs. 5.9%, and 13.5% vs. 7.6%, all p<0.001) compared to controls.
CONCLUSIONS: Our analysis suggests male ever-smokers aged 45-64, and male never-smokers 65-75 and >75 years old, have a >1% prevalence of AAA, and therefore could benefit from screening. When these groups were compared to well-matched controls, significantly greater mortality was observed, indicating the possibility of aneurysm-related mortality. 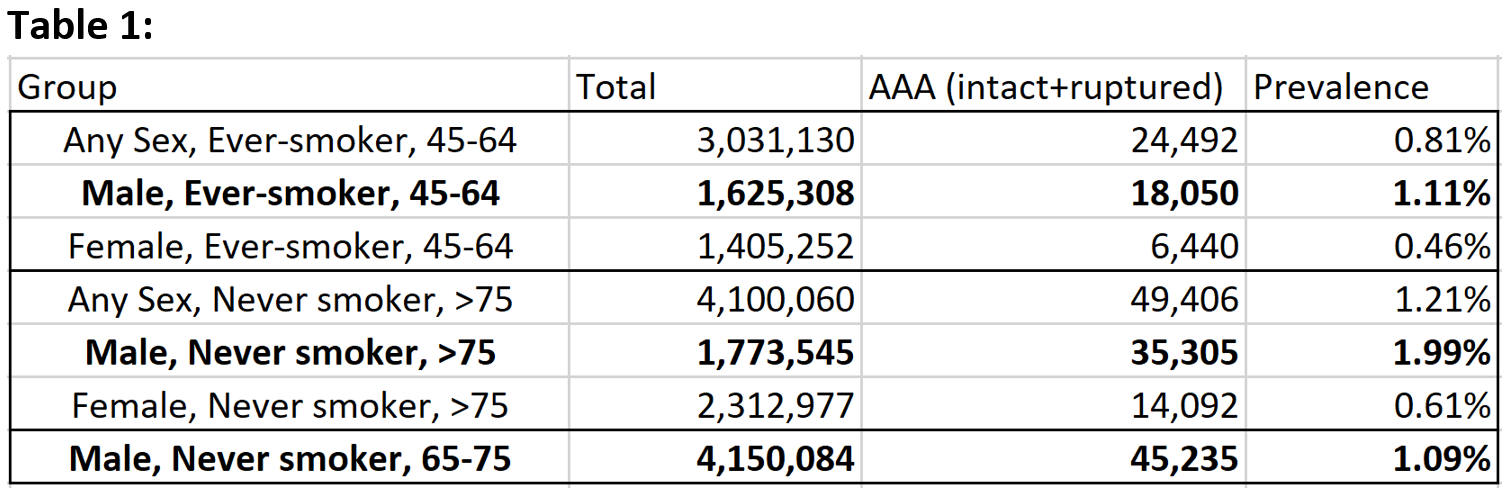
Back to 2022 ePosters