
Stroke Risk In Transfemoral Carotid Artery Stenting With And Without Distal Embolic Protection
Sophie X. Wang, MD1, Christina L. Marcaccio, MD, MPH1, Priya B. Patel, MD, MPH1, Kristina A. Giles, MD2, Peter A. Soden, MD3, Marc L. Schermerhorn, MD1.
1Beth Israel Deaconess Medical Center, Boston, MA, USA, 2Maine Medical Center, Portland, ME, USA, 3Brown University, Providence, RI, USA.
Objectives: Despite current guidelines recommending the use of distal embolic protection during transfemoral carotid stenting (tfCAS) to prevent periprocedural stroke, there remains significant variation in the use of distal filters. We sought to assess in-hospital outcomes in patients undergoing tfCAS with and without a filter for distal embolic protection.
Methods: We identified all patients undergoing tfCAS in the VQI from March 2005-February 2021 and excluded those who received proximal embolic balloon protection. We stratified patients by symptom status and created propensity score-matched cohorts of patients who underwent tfCAS with and without placement of a distal filter. We performed subgroup analysis of patients with failed vs successful filter placement. In-hospital outcomes were assessed using log binomial regression, adjusted for protamine use. Outcomes of interest were composite stroke/death, stroke, death, myocardial infarction (MI), transient ischemic attack (TIA), and hyperperfusion symptoms.
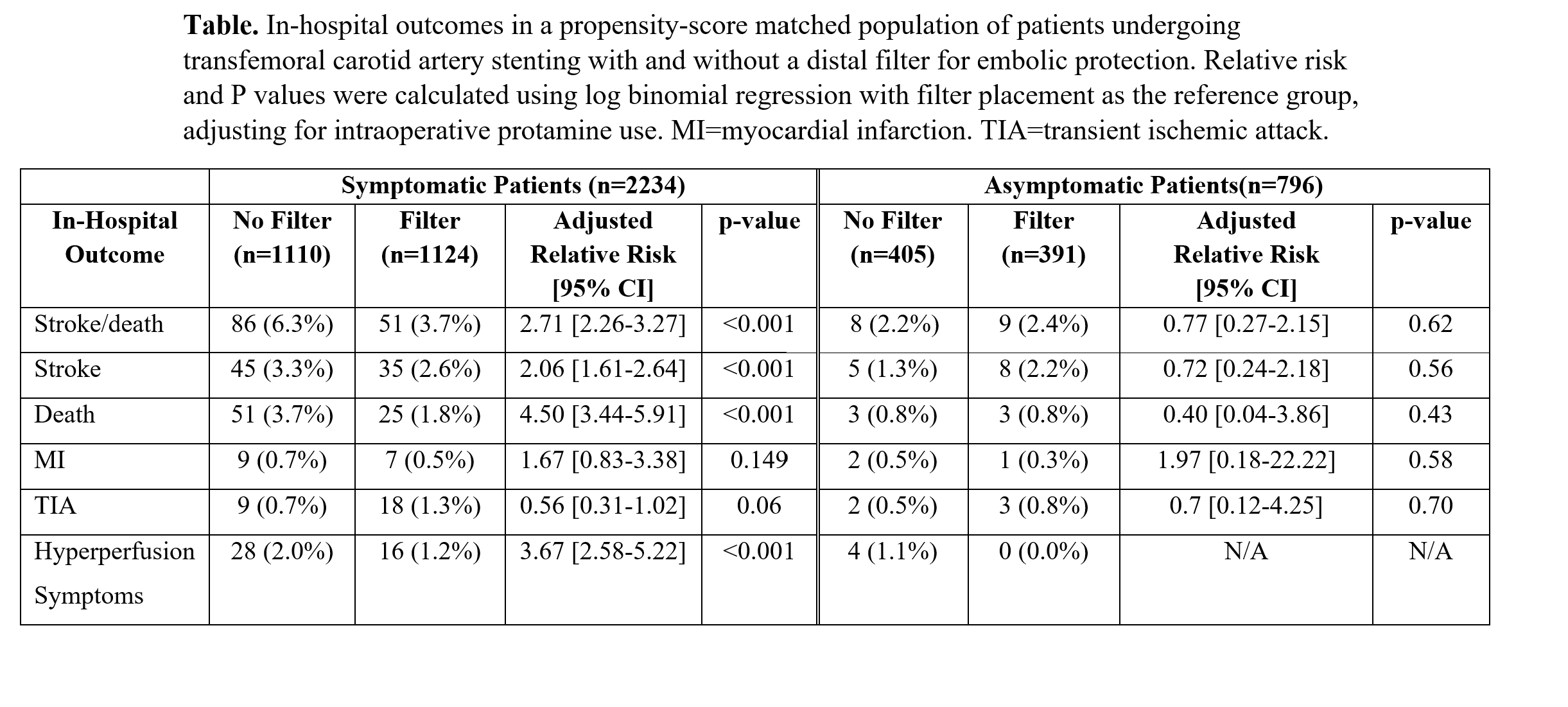
Results: Among 26,511 patients who underwent tfCAS, 24,480(92%) had a filter placed for distal embolic protection and 2031(8%) did not. In 2742 matched symptomatic patients, no filter was associated with higher rates of stroke/death (no filter:6.3% vs filter:3.7%, adjusted relative risk [aRR]:2.71[2.26-3.27]), stroke (3.3% vs 2.6%, aRR:2.06[1.61-2.64]), death (3.7% vs 1.8%, aRR:4.50[3.44-5.91]), and hyperperfusion symptoms (2.0% vs 1.2%, aRR:3.67[2.57-5.23])(Table). In 742 matched asymptomatic patients, there were no differences in outcomes between groups (stroke/death: 2.2% vs 2.4%, aRR:0.77[0.27-2.15]; stroke: 1.3% vs 2.2%, aRR:0.72[0.24-2.18]; death: 0.8% vs 0.8%, aRR:0.40[0.04-3.86]; hyperperfusion: 1.1% vs 0%, aRR N/A)(Table). In a secondary analysis of 1,116 matched patients who had failed attempt at filter placement versus successful filter placement, there was a trend toward higher stroke/death with failed filter placement (5.7% vs 3.4%, aRR:1.68[0.95-2.85]). Failed filter placement was associated with higher stroke rates (5.2% vs 2.2%, aRR:2.27[1.17-4.40]), but there were no differences in death or hyperperfusion symptoms between groups.
Conclusions: TfCAS without distal embolic protection was associated with >50% higher risk of in-hospital stroke and death in symptomatic patients. These findings support current SVS guidelines recommending routine use of distal embolic protection in this population. Further studies are needed to define the risks and benefits of filter placement in asymptomatic patients.
Back to 2022 ePosters