
Thoracoabdominal Aortic Thrombus Extending Into Visceral Branches
Akiko Tanaka, MD, PhD, Hazim J. Safi, MD, Arash Keyhani, DO, Kourosh Keyhani, DO.
McGovern Medical School at UTHealth, Houston, TX, USA.
DEMOGRAPHICS: A 42-year-old female presents with acute epigastric abdominal pain. She has an elevated white blood cell count of 19.4x109/L and lactic acid of 3.8 mmol/L. Pedal pulses were palpable bilaterally. The patient has pain out of proportion in the upper abdomen to the right flank without rebound or guarding.
HISTORY: Patient is a 42-year-old obese black female with a past medical history of hypothyroidism, hypertension, diabetes, chronic anemia, and history of thrombus in the descending thoracic aorta treated with anticoagulation 14 months ago, who presents with a one-day history of epigastric abdominal pain. She was taken off the anticoagulation after confirming the resolution of the thrombus 13 months ago. Patient reports the pain was initially intermittent but became more intense and persistent. Subsequent imaging showed thoracoabdominal aortic thrombus extending to the celiac artery and superior mesenteric artery.PLAN: We planned for percutaneous pharmaco-mechanical thrombectomy for the celiac axis with distal protection, exploratory laparotomy for open embolectomy of the superior mesenteric artery and open thrombectomy of the thoracoabdominal aorta through infrarenal aortotomy. All the bowels were viable and the patient was discharged home on the postoperative day 6 on apixaban.
DISCUSSION: Aortic Mural thrombus can be treated with systemic anticoagulation but some may persist and require surgical intervention. There are increasing number of total percutaneous approach to treat the aortic mural thrombus, however, in the setting of such as the current case suspicious for ischemic bowel, hybrid approach may be beneficial. 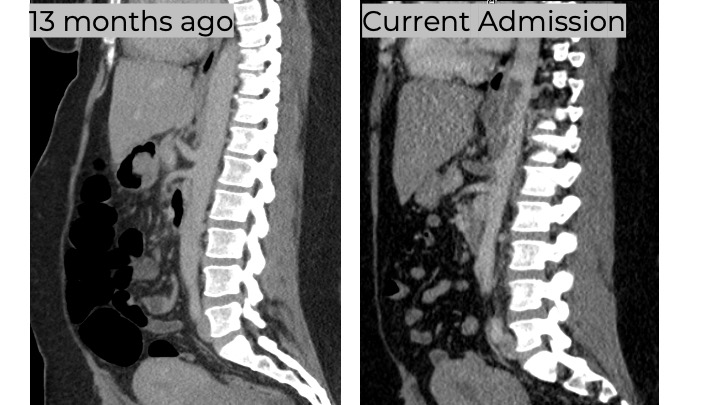
Back to 2022 Abstracts