
Emergent Endovascular Repair Of A Tracheo-innominate Fistula
Aaron Hayson, MD, Thomas Hawken, MD, Hernan Bazan, MD.
Ochsner Medical Center, New Orleans, LA, USA.
DEMOGRAPHICS: 67-year-old male with history of laryngeal cancer. HISTORY:The patient received radiation and had partial obstruction of his airway requiring a tracheostomy. He presented with large volume hemoptysis from the tracheostomy and sustained pulseless electrical activity (PEA) arrest; return of spontaneous circulation (ROSC) was achieved after 2 rounds of ACLS. He once again had massive bleeding from his tracheostomy site and another PEA arrest but had ROSC after one more round of ACLS. A tracheo-innominate fistula diagnosis was made and an emergent operative repair planned. PLAN:The patient had multiple herald bleeds from a tracheo-innominate fistula the decision was made to proceed with emergent salvage therapy. Cardiac Surgery felt he was not a candidate for a median sternotomy approach for direct repair due to his prior history of radiation to his neck and chest. Hence, the patient was brought to a hybrid operating room for evaluation and treatment. DISCUSSION:
Computed tomography angiography (CTA) demonstrated a bovine arch and hemorrhage appeared to be coming from the confluence of the innominate to the right carotid and subclavian arteries. An endovascular approach entailing exclusion of this confluence using ‘kissing’ covered stents was then planned. As predicted on pre-operative 3D CTA reconstruction, the tracheostomy lay in close proximity to the bifurcation of the innominate and right common carotid artery (Fig. 1A). Wire access into the right external carotid artery and thyrocervical trunk was established (Fig. 1B). An 8 x 79mm covered balloon-expandable stent (VBX) was placed into the right common carotid artery, which measured 8mm, and an 11 x 59mm VBX stent was advanced into the right subclavian artery, which measured 13mm (Fig. 1C). Both stents were positioned so that half of the stent length was in the innominate artery, which measured 16mm. Using an ‘eye of the tiger’ technique, the balloon expandable stents were deployed and molded to seal the right common carotid, right subclavian, innominate arteries; the distal right subclavian stent was dilated to 13mm. Completion angiogram revealed flow through both stents (Fig. 1D). Percutaneous closure of the 8fr sheath was achieved the patient recovered and was discharged on post-operative day #4. 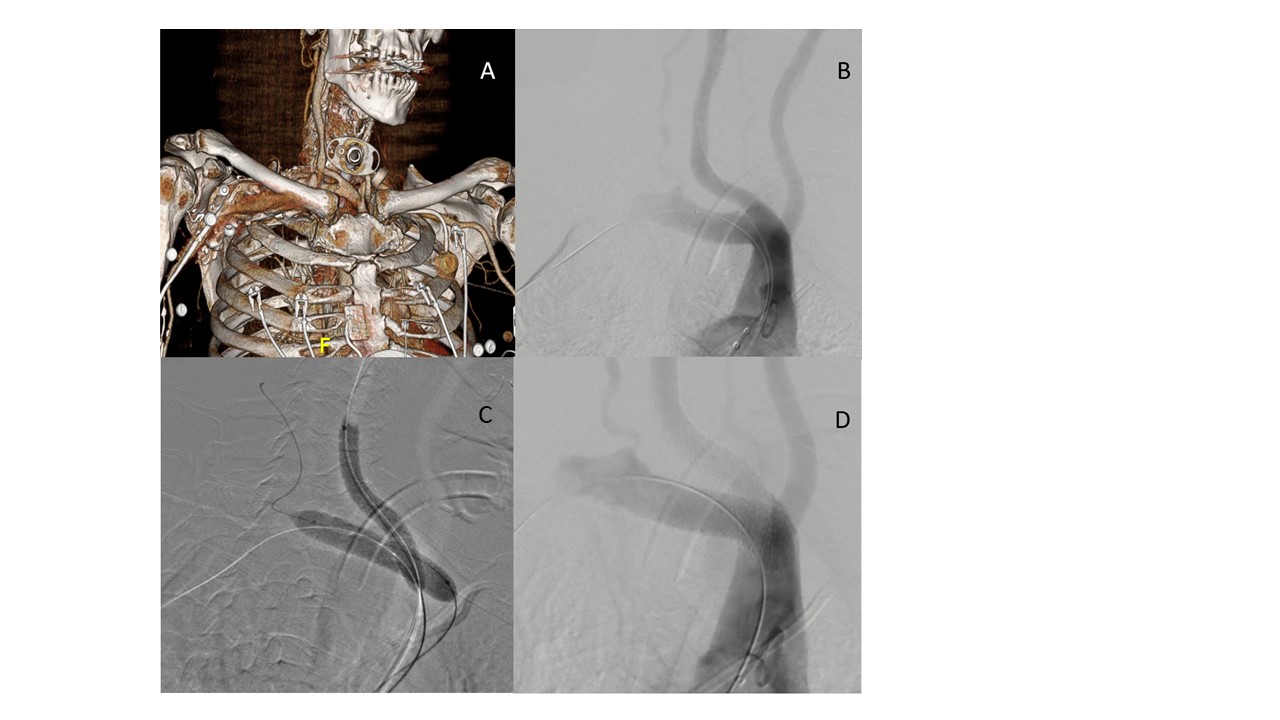
Back to 2022 Abstracts