
30 Year Old Man With A Symptomatic Fractured Iliac Venous Stent
Indrani Sen, Manju Kalra.
Mayo clinic, Rochester, MN, USA.
DEMOGRAPHICS The patient is a 30 year-old male presenting with recurrent venous claudication. HISTORY The patient presented with recurrent left lower extremity (LLE) exertional fatigue with jogging 2 years following left external iliac (EIV) - common femoral vein (CFV) stenting elsewhere in 2017 with a 16 x 100 mm Venovo stent. He denied a history of venous thromboembolic events. Physical examination revealed increased circumference and tightness of the left thigh and calf with no signs of chronic venous stasis and normal arterial pulses. Duplex ultrasound (DUS) revealed venous stent fracture with nonocclusive in-stent thrombosis causing high grade stenosis. CT venogram (CTV) revealed extensive peri-arterial soft tissue thickening surrounding the common femoral artery without FDG uptake on PET/CT scan. Distally the stent extended across a patent, stenosed saphenofemoral junction. LLE femoropopliteal veins were patent. PLAN Open surgical intervention was performed. Extensive left iliofemoral exploration revealed intense scarring with a dense inflammatory rind deep to inguinal ligament at the site of compression fracture of the iliofemoral stent. Proximal and distal iliofemoral venous control was obtained. The metal structure of the Venovo stent was noted to extend through the entire thickness of the vein wall and into the ilio-femoral arterial wall. Right great saphenous vein was harvested endoscopically, fashioned into a spiral graft over a 32-Fr mandril and implanted as an interposition ilio-femoral venous graft after excision of a 4-cm segment containing the crushed, stent, leaving patent proximal EIV and distal CFV stent in situ. A short segment of ilio-femoral artery injured by the crushed stent was replaced with an interposition left basilic vein conduit, protected by interposing a bovine pericardial patch wrap around the remnant stented EIV. Completion intraoperative and postoperative DUS and CTV confirmed patency of the reconstructions. LLE tightness/ swelling improved significantly. He required wound hematoma evacuation on POD 4 but was discharged on therapeutic anticoagulation without further incident. He remains asymptomatic with full aggressive activity with patent reconstructions 1 year later (Fig 1). DISCUSSION Newer venous stents with greater radial force may suffer compression deep to the inguinal ligament. Open reconstruction required is challenging. 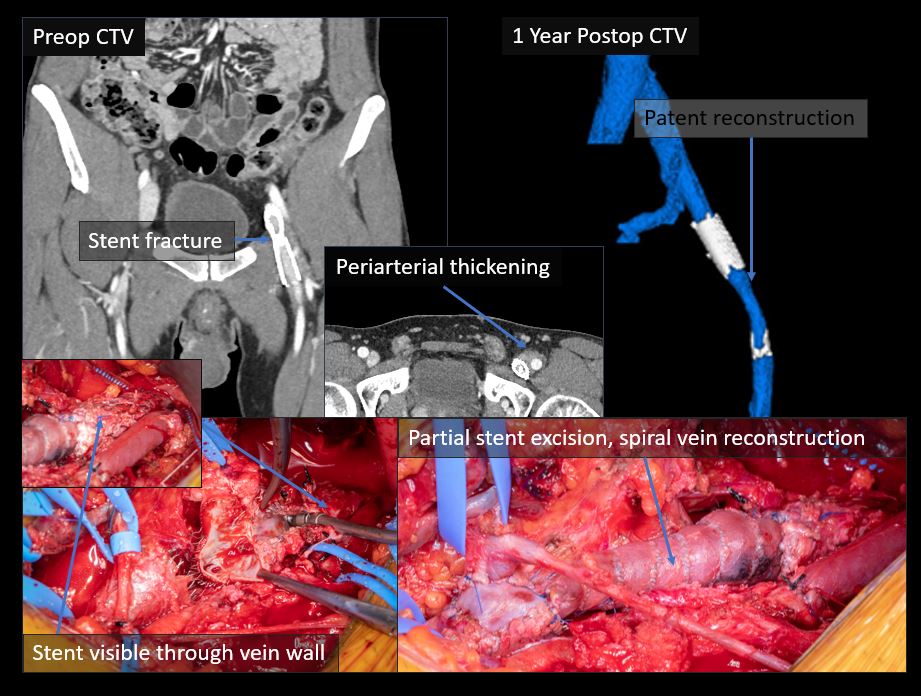
Back to 2022 Abstracts