Back to 2024 Display Posters
Lower Extremity Malperfusion From Blunt Type B Aortic Dissection
Andrew Youssef, MD1, Neil Desai, DO
1, Eric Trestman, MD
1, Stuart Harlin, MD
2, Ray Hunter, MD
1.
1HCA Houston Healthcare: Kingwood, Kingwood, TX, USA,
2McGovern Medical School at The University of Texas Health Science Center at Houston, Houston, TX, USA.
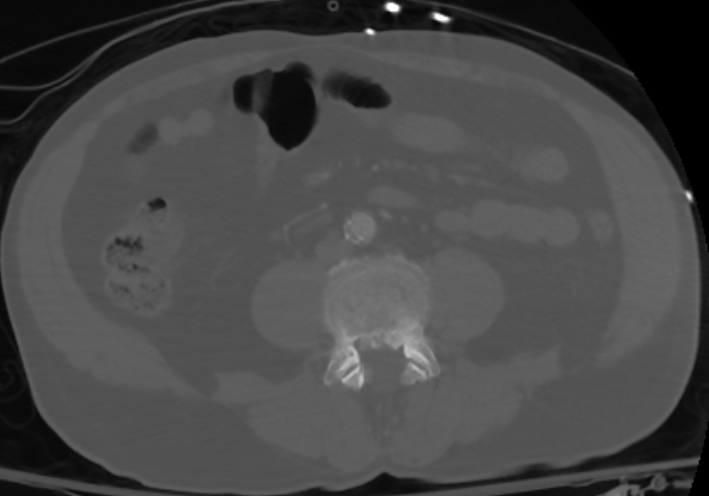
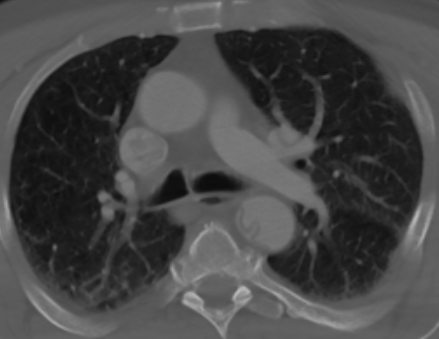
DEMOGRAPHICS: Blunt traumatic aortic injury (BTAI) remains the second leading cause of mortality in non-penetrating traumas. Typically graded from 1 to 4, we present a case with a complicated type B aortic dissection.HISTORY: The patient is a 64-year-old male with history of hypertension and COPD who initially as a level I trauma following a fall from greater than 25 feet with complaints of chest pain and pulseless right lower extremity. Computed Tomography revealed a Type-B aortic dissection with extension of the dissection flap extending from the left subclavian artery and into the right common iliac artery. PLAN: The patient was taken to the hybrid operating room with plans for thoracic endovascular aortic repair (TEVAR). The true lumen was believed to be accessible via right femoral access, percutaneous access and closure was performed with a pigtail catheter advanced through the true lumen to the ascending aorta. Aortography and intravascular ultrasound (IVUS) confirmed that we were within true lumen throughout. Patient underwent emergent thoracic endovascular aortic repair using Cook Alpha TEVAR device 32 mm x 109 mm sparing the left subclavian artery. IVUS noted continued compression of the visceral segment and right common iliac artery with distal extension using Cook dissection stent 36 mm x 180 mm then performed to the level of the celiac artery. Completion IVUS was performed revealing excellent remodeling throughout the visualized portions of the aorta with only minimal false lumen remaining within the abdominal segment. The previous iliac occlusion was noted to have resolved after thoracic endovascular aortic repair. Completion angiography revealed excellent flow through the true lumen and patency of all visceral vessels and lower extremity arteries. Percutaneous closure was performed with intact pulses noted distally. Follow-up imaging has noted positive aortic remodeling. At this time the patient has returned to his normal activities without limitations.



Back to 2024 Display Posters