Back to 2024 Display Posters
Comparative Assessment Of Risk Score Performance For Predicting Post Ruptured Abdominal Aortic Aneurysm Repair Mortality: An In-depth Analysis In The NSQIP And VQI Registries
Andrew S. Warren, BS1, Elina Quiroga, MD
1, Thomas FX O'Donnell, MD
2, Marc L. Schermerhorn, MD
3, Sara L. Zettervall, MD, MPH
1, Kirsten Dansey, MD, MPH
1.
1University of Washington Division of Vascular Surgery, Seattle, WA, USA,
2Division of Cardiac, Thoracic, and Vascular Surgery, New York-Presbyterian Columbia University Medical Center, New York, NY, USA,
3Division of Vascular and Endovascular Surgery, Beth Israel Deaconess Medical Center, Boston, MA, USA.
OBJECTIVES: Several risk scores are currently available to predict patient survival of a ruptured abdominal aortic aneurysm repair (rAAA). This study aims to assess and compare the performance of commonly used risk scores by means of NSQIP and Vascular Quality Initiative (VQI) quality improvement registries.
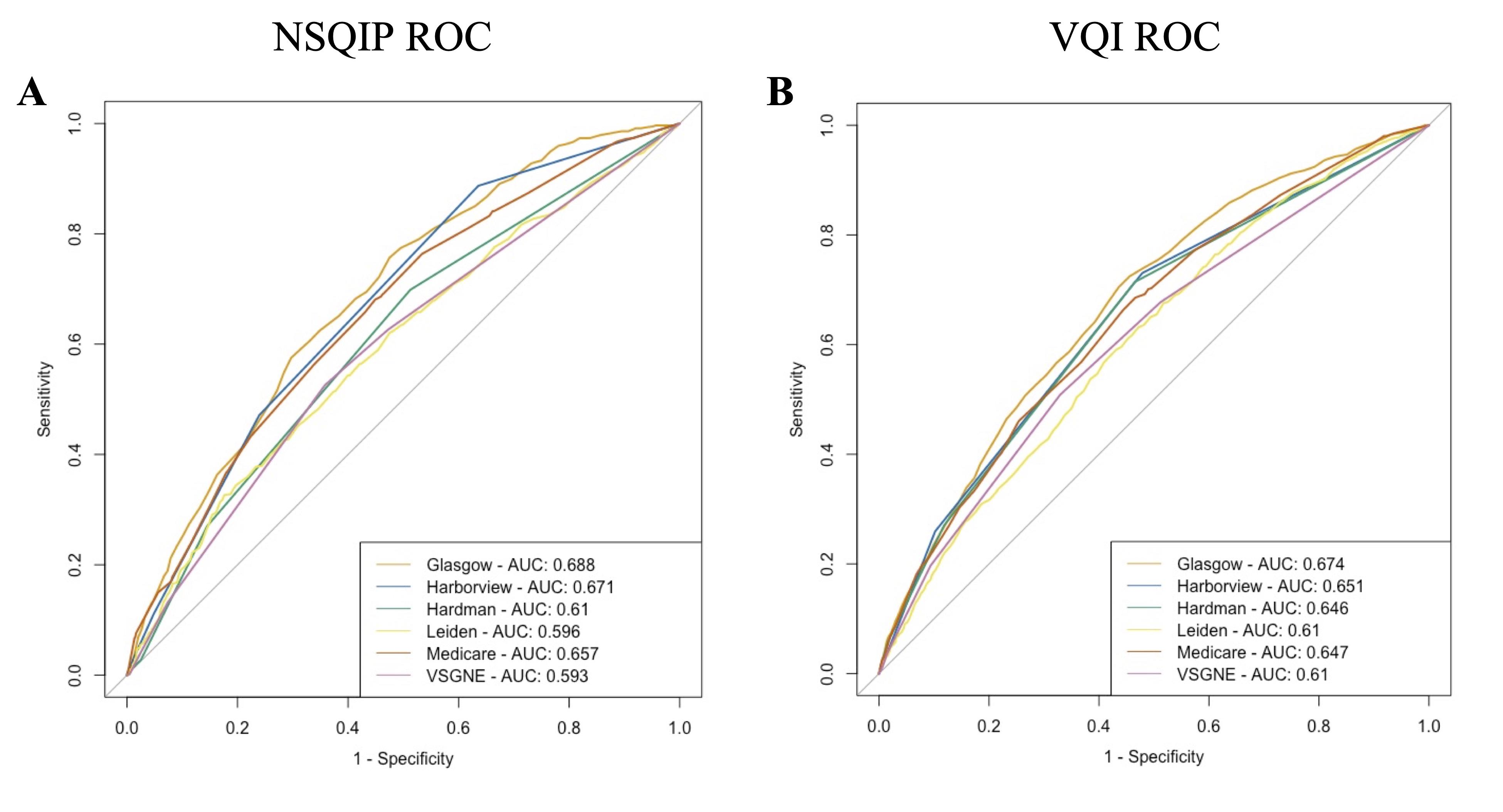
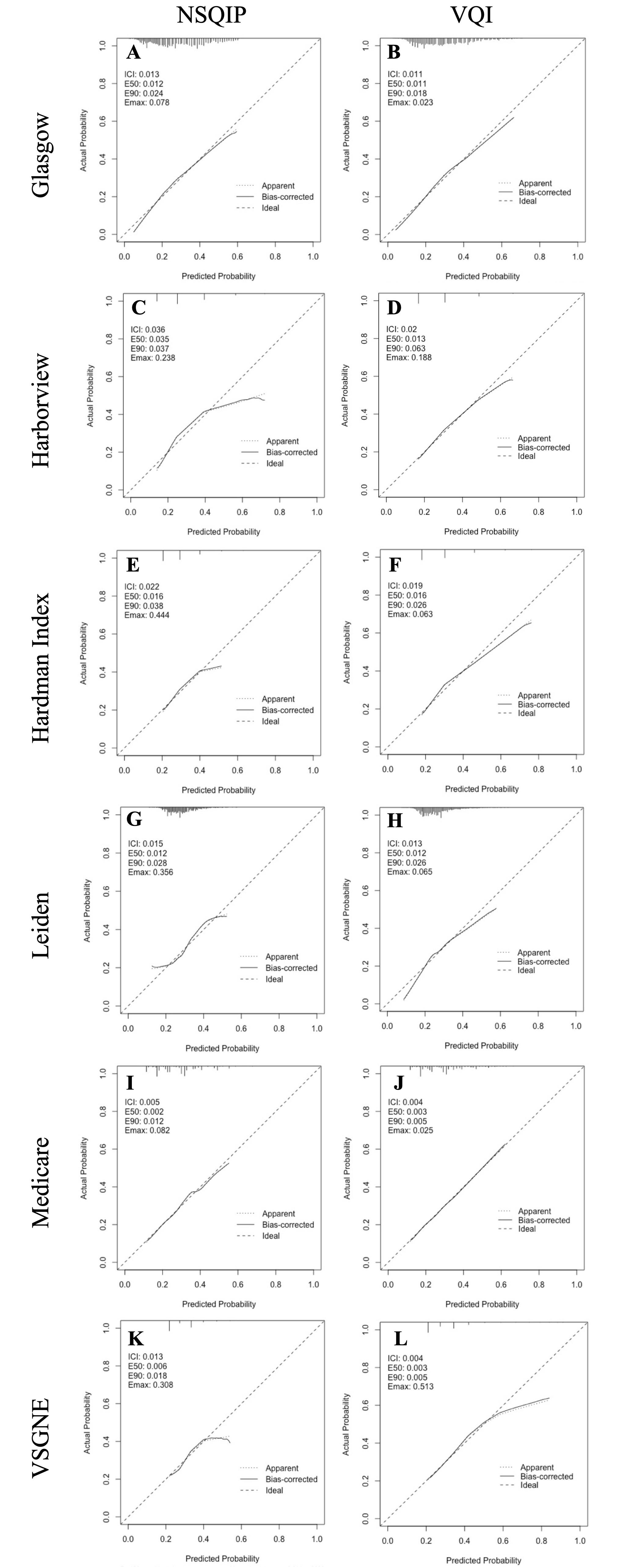
METHODS: All patients who underwent rAAA repair in NSQIP and VQI were included. The following risk scores were calculated: Glasgow Aneurysm Score (GAS), modified Harborview Risk Score (HRS), Hardman Index (HI), Leiden Score, Medicare Risk Score, and the Vascular Surgery Group of New England risk score (VSGNE). Using 30-day mortality as the primary outcome, receiver operating characteristic area under the curves (AUC) were calculated for each risk score. Discrimination was compared within datasets using the Delong test. Calibration was assessed using graphical calibration curves and quantified via the integrated calibration index (ICI).
RESULTS: 2134 patients were identified in NSQIP and 6458 in VQI. In both NSQIP and VQI, the GAS demonstrated superior discrimination ability (AUC 0.69 NSQIP, 0.67 VQI) compared to all other risk scores (p<0.01 vs all; Fig 1). The modified HRS (AUC 0.67 NSQIP, 0.65 VQI) and Medicare risk score (AUC 0.66 NSQIP, 0.65 VQI) were comparable to each other (p=0.37 NSQIP, p=0.54 VQI) and followed the GAS in discrimination ability. The Medicare risk score was best calibrated as shown by its close adherence to a 45-degree line on both calibration curves (ICI 0.005 NSQIP, 0.004 VQI). All measures besides the Medicare risk score overestimated risk at the extremes (Fig 2). The modified HRS and HI were the most applicable pre-operatively given their reliance exclusively on routinely collected labs and vitals.
CONCLUSIONS: The Glasgow Aneurysm Score displayed superior ability to discern between high- and low-risk ruptured AAA patients. The Medicare risk score was best calibrated in its ability to precisely predict mortality risk. The modified Harborview Risk Score showed a combination of acceptable discrimination and calibration while relying only on routinely collected labs and vitals, affording it improved applicability.


Back to 2024 Display Posters