Back to 2024 Display Posters
Optimal Egfr Cutoffs For Risk Of Death Or Dialysis After Open And Endovascular Abdominal Aortic Aneurysm Repair
Elisa Caron, MD1, &#
8239;Sai Divya Yadavalli, MD
1, Roger Davis, ScD
1, Mark Conrad, MD
2, Virendra Patel, MD
3, Marc Schermerhorn, MD
1.
1Beth Israel Deaconess Medical Center, Boston, MA, USA,
2St Elizabeth's Medical Center, Boston, MA, USA,
3New York Presbyterian/Columbia University Medical Center, New York, NY, USA.
OBJECTIVES: Chronic kidney disease (CKD) is known to increase morbidity and mortality for both open and endovascular repair of AAA. However, a binary classification of estimated glomerular filtration rate (eGFR) < 60 may not be the optimal cutoff.
METHODS: Vascular Quality Initiative (VQI) databases for intact, first-time Open Aneurysm repair (OAR) and EVAR were analyzed from 2013-2023 and divided into cohorts based on eGFR (≥60, 45-59, 30-44, <30 ml/min/1.73m
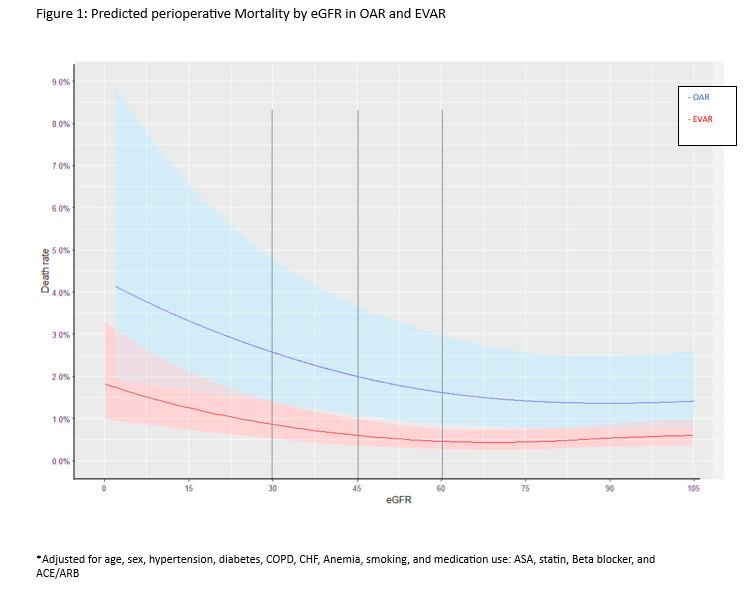
2). Chi-square and linear regression analysis were used to compare perioperative mortality and rates of requiring permanent hemodialysis (HD), with eGFR ≥60 cohort as the reference. A Linear Regression model with a restricted cubic spline configuration was used to provide a visual representation of the relationship between eGFR and predicted perioperative mortality. (Figure 1)
RESULTS: Compared to patients with eGFR ≥60, patients with eGRF 45-59 had similar adjusted odds of mortality for both OAR and EVAR (OAR: 4.9% vs 3.1%, aOR 1.1[95% CI 0.81,1.49];p>0.05 and EVAR: 1.0% vs 0.8%, aOR 1.01 [0.79, 1.28];p>0.9). Those in the 30-44 group demonstrated increased odds of mortality (OAR: 6.6%, aOR 1.3[0.92,1.81]; p=0.12, EVAR: 1.7%,1.35[1.05,1.72];p= 0.015), and patients with eGFR <30 demonstrated the highest odds of mortality at (OAR: 3.4% aOR 2.26[1.54,3.25];p<0.001, EVAR: 11.5%, aOR 2.3[1.78,2.97];p<.001).
Permanent dialysis requirement followed a similar trend with the odds of permanent dialysis increasing as eGFR decreased. Compared to the
>60 group, those in the eGFR 45-59 group had similar rates of permanent HD, (OAR, 1.3% vs 0.8%, aOR 1.49, [0.82,2.61]; P=0.2; EVAR: 0.1% vs 0.1%, aOR 1.09[0.39,2.58];p=0.2). Patients in the 30-44 group showed a small change in dialysis requirement, (OAR: 1.1%. aOR1.18[0.53-2.39]; p=0.7,EVAR: 0.3%, aOR 3.59[1.73-7.24]; p<.001). As with perioperative mortality greatest differences were seen in the <30 group (OAR: 4.2% aOR 4.14[2.15, 7.62] p<0.001, EVAR: 1.5%, aOR 18.1[10.1,33.1]; p<.001) further highlighting the significant variation in outcomes among patients with eGFR
<60.
CONCLUSIONS: Rather than a binary eGFR cutoff of <60 to stratify patient risk after AAA repair, a better understanding of perioperative risk may be achieved by stratifying into 3 groups of 45-59, 30-44, and <30.

Back to 2024 Display Posters