Back to 2024 Display Posters
Treatment Algorithm And Results For Ascending And Aortic Arch Pathologies In Patients Who Cannot Tolerate Open Surgery
Meiyi Shi, MD, Anjali Ratnathicam, DO, David O'Connor, MD, Yuriy Dudiy, MD, George Batsides, MD, Mark Anderson, MD, Michael Wilderman, MD.
Hackensack University Medical Center, Hackensack, NJ, USA.
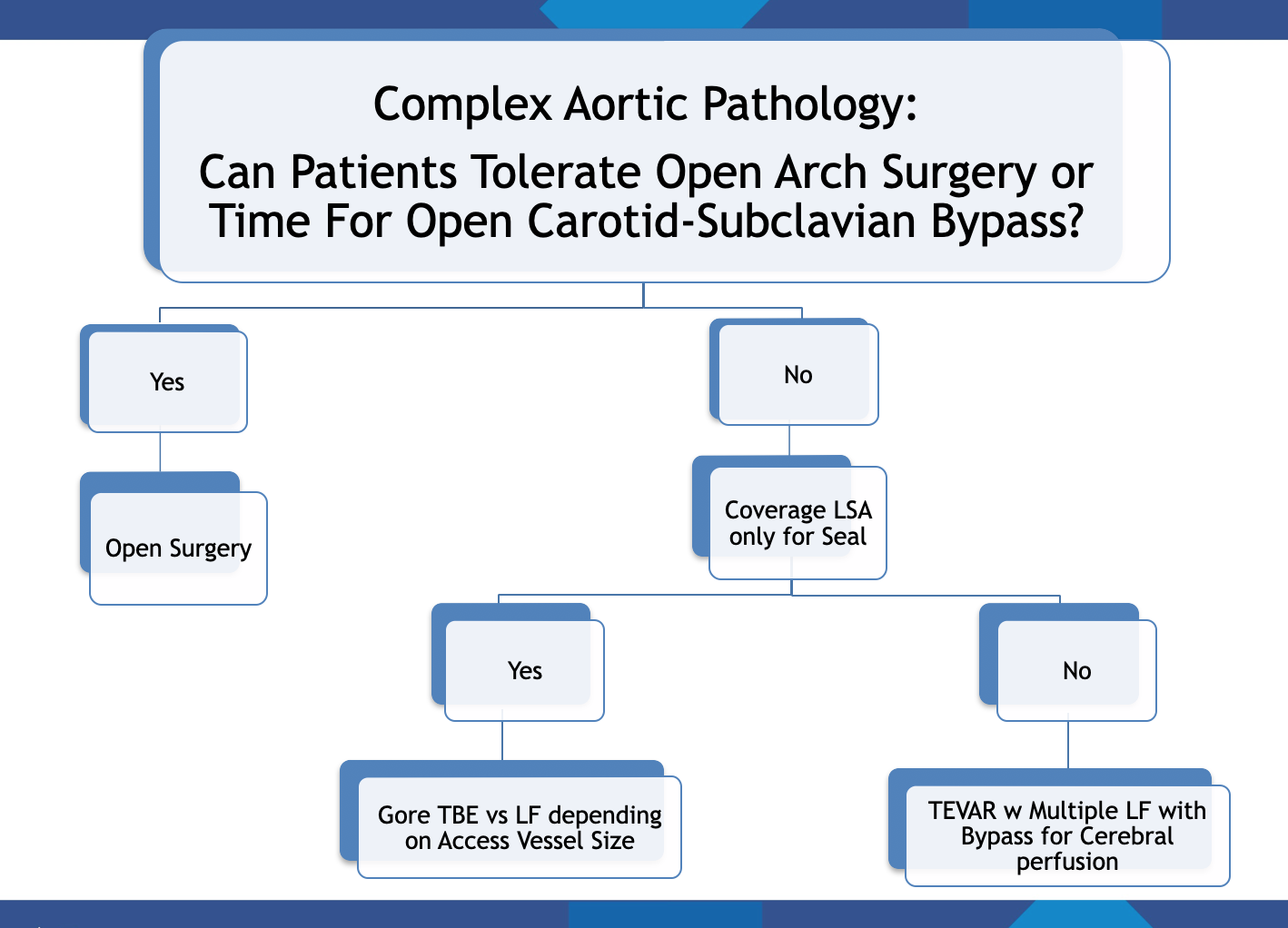
OBJECTIVES: TEVAR has emerged as the first-line therapy for most distal arch and descending aortic pathologies. For more proximal pathologies, open surgery remains the standard. TEVAR with zone 2 landing mandates left subclavian artery (LSA) coverage, which often then necessitates surgical revascularization using carotid-subclavian bypass or transposition. This is associated with longer operative time, lengthened hospitalizations, and increased complications. GORE TAG thoracic branch endoprosthesis (TBE) is a first-of-its-kind FDA approved device designed for zone 2 TEVAR with preservation of LSA. For more proximal arch diseases, there is no commercially available device to treat patients who cannot undergo arch reconstructions. TEVAR with in-situ laser fenestration (LF) could present a safe endovascular alternative for patients who cannot tolerate open procedures.
METHODS: Since May 2022, we have performed 10 TBE and 14 TEVARs with LF of one or more of the arch vessels to treat complex ascending and arch aortic diseases. We reviewed both techniques retrospectively for technical success defined by proximal seal, along with in-hospital and 30-day mortality. Length of stay and incidence of major adverse events (MAE) such as MI, respiratory failure, bowel ischemia, stroke, renal failure, and paralysis were examined in comparison to historic controls. Patients were followed for presence of an endoleak, increase in aortic size, and freedom from intervention.
RESULTS: Technical success for both TBE and LF was 100% with no Type 1, 2, or 3 endoleaks detected on completion angiogram. All except one patients treated with TBE were discharged on postoperative day 1. There was no incidence of MAE, re-intervention, or mortality within the short term period for TBE; one incidence of stroke and one incidence of death were noted for LF. Early postoperative imaging (< 6 months) showed excellent aortic aneurysm or dissection exclusion, along with 100% patency of the side branches.
CONCLUSIONS: Following our treatment algorithm, we showed favorable results using TBE or LF for successful and safe single stage treatment of complex thoracic aortic diseases. While these early results are promising, no one technique is perfect for all situations and more follow up and longer term data is required.

Back to 2024 Display Posters